Highlights
|
Goals
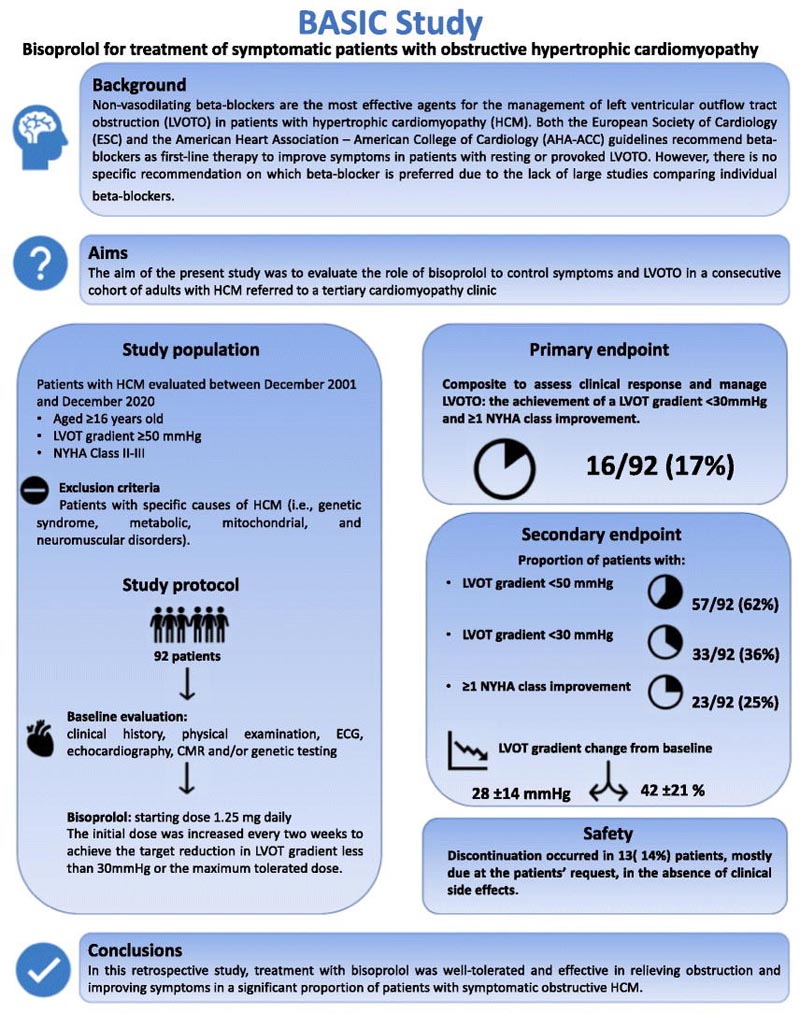
To evaluate the role of bisoprolol in the control of symptoms and left ventricular outflow tract obstruction (LVOTO) in a consecutive cohort of adults with hypertrophic cardiomyopathy (HCM).
Methods and results
In this retrospective study, HCM patients with an LVOT gradient ≥50 mmHg after the Valsalva maneuver and New York Heart Association (NYHA) class II-III symptoms were assigned to receive bisoprolol (starting at 1.25 mg daily).
The initial dose was increased every two weeks to achieve the target gradient of LVOT <30 mmHg or the maximum tolerated dose. The primary endpoint was achievement of an LVOT gradient <30 mmHg and NYHA class improvement ≥1.
Secondary endpoints were the proportion of patients with an LVOT gradient <30 mmHg or <50 mmHg, the proportion of patients with NYHA class improvement ≥1, and the change from baseline in LVOT gradient.
Between December 2001 and December 2020, 92 patients were enrolled in the study. Sixteen (17%) patients on bisoprolol had the primary endpoint.
Bisoprolol reduced the LVOT gradient to less than 30 mmHg in 33 (36%) patients, to less than 50 mmHg in 57 (62%), and improved NYHA class in 30 (33%).
The mean LVOT gradient reduction with bisoprolol was 28 (±14) mmHg and the percentage reduction was 42 (±21)%.
In 35 (38%) patients, bisoprolol did not reduce the gradient to less than 50 mmHg, requiring disopyramide and/or myectomy to achieve this goal.
Conclusion
Bisoprolol treatment was well tolerated and effective in relieving obstruction and improving symptoms in a significant proportion of patients with symptomatic obstructive HCM.















