
In the Regeneron monoclonal combination of the seronegative group: - Reduction in deaths (24% vs 30%, RR 0.80, p = 0.001) - Reduction in length of hospital stay (median 13 vs. 17 days) - Reduced risk of going to a mechanical ventilator or dying (30% vs 37%, RR 0.83, 95% CI 0.75-0.92) Effect observed in all pre-specified subgroups, e.g. e.g. effect observed in seronegative people regardless of age, sex, time since the onset of the disease, severity, etc. No benefits were observed in the general population combining seronegative (32%), seropositive (54%) and unknown serostatus (14%) patients. This is the first demonstration of an antiviral reducing mortality in hospitalized patients with COVID-19. 1. Other medication available to treat severe COVID. 2. Proof of principle for monoclonals specifically and antivirals in general in severe COVID. Sir Peter Horby |
The Randomized Evaluation of COVID-19 Therapy (RECOVERY) trial has shown that the investigational antibody combination developed by Regeneron reduces the risk of death when given to hospitalized patients with severe COVID-19 who have not generated a natural antibody response of their own .
The treatment uses a combination of two monoclonal antibodies (casirivimab and imdevimab, known as REGEN-COV in the US) that specifically bind to two different sites on the coronavirus spike protein, neutralizing the virus’s ability to infect cells.
Previous studies in non-hospitalized COVID-19 patients have shown that treatment reduces viral load, shortens time to symptom resolution, and significantly reduces the risk of hospitalization or death.
In a small trial in hospitalized patients, preliminary evidence suggested a clinical benefit in patients who had not mounted a natural antibody response of their own when they entered the trial (they were seronegative). RECOVERY is the first trial large enough to definitively determine whether this treatment reduces mortality in hospitalized patients with severe COVID-19.
Between September 18, 2020 and May 22, 2021, 9,785 hospitalized patients with COVID-19 were randomly assigned to receive usual care plus combination antibody therapy (casirivimab 4g with imdevimab 4g by intravenous infusion) or routine care. routine alone as part of the RECOVERY trial.
Of these, approximately one-third were seronegative at baseline (i.e., they had not mounted a natural antibody response of their own), half were seropositive (i.e., they had already developed natural antibodies), and one-sixth had unknown serostatus.
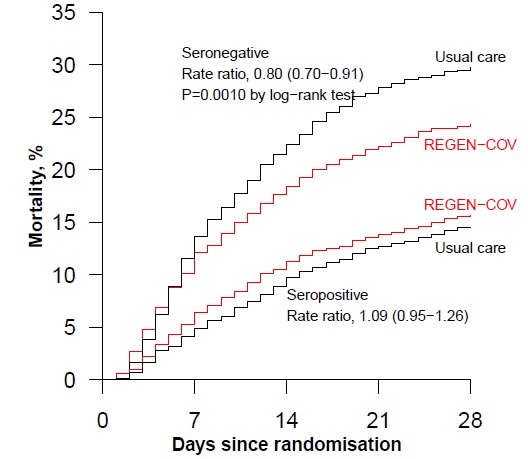
Among patients who received usual care only, 28-day mortality was twice as high in those who were seronegative (30%) versus those who were seropositive (15%) at study entry.
Follow-up is complete for 99% of participants and preliminary results were announced today.
Among patients who were seronegative at baseline (the primary analysis population for this comparison), the antibody combination significantly reduced the primary outcome of 28-day mortality by one-fifth compared with usual care alone (24%). of patients in the antibody combination group died vs 30% of patients in the usual care group; rate ratio 0 80; 95% confidence interval 0 70-0 91; p = 0 001 ).
Therefore, for every 100 of these patients treated with the antibody combination, there would be six fewer deaths.
There was clear evidence that the treatment effect in seronegative patients differed from that in seropositive patients (heterogeneity test p = 0.001).
When combining the larger seropositive group (as well as those with unknown status) with the seronegative patients, there was no longer a significant effect on 28-day mortality (overall, 20% of patients in the antibody combination group died versus 21% of patients in the usual care group; rate ratio 0·96; 95% confidence interval 0·86–1·03; p = 0·17).
For seronegative patients, the length of hospital stay was four days shorter (median 13 days vs. 17 days) among those assigned to the antibody combination than the usual care group, and the proportion of patients discharged alive on day 28 it was higher (64% vs. 58%; rate ratio 1·19, 95% confidence interval 1·08 to 1·30).
Among seronegative patients who did not receive invasive mechanical ventilation at baseline, the risk of progressing to the combined endpoint of invasive mechanical ventilation or death was lower among those assigned to the antibody combination than the usual care group (30% vs. to 37%; hazard ratio 0·83, 95% confidence interval: 0·75 to 0·92).
No such benefits were observed in the overall study population (combining patients with negative, positive, or unknown HIV status).
Comments
Sir Peter Horby , Professor of Emerging Infectious Diseases at the Nuffield Department of Medicine, University of Oxford, and deputy chief investigator of the RECOVERY trial, said: “These results are very interesting. The hope was that by administering a combination of antibodies targeting the SARS-CoV-2 virus we could reduce the worst manifestations of COVID-19. However, there was great uncertainty about the value of antiviral therapies in late-stage COVID-19 disease. "It is wonderful to know that even in cases of advanced COVID-19 disease, attacking the virus can reduce mortality in patients who have failed to generate an antibody response of their own."
Sir Martin Landray , Professor of Medicine and Epidemiology at the Nuffield Department of Population Health, University of Oxford, and Deputy Chief Investigator, said: ``We now know that this combination of antibodies is not only bad for the virus, but It is also good for the sickest, patients who have not managed to mount their own natural immune response. That’s excellent news: It’s the first time that an antiviral treatment has been shown to save lives in patients hospitalized with COVID-19. "We are incredibly grateful to the NHS staff and patients who have contributed to today’s discovery."
RECOVERY participant Kimberley Featherstone (37) was treated at Huddersfield Royal Infirmary and Calderdale Royal Hospital and randomized to the monoclonal antiviral antibody combination. She said: “I was certainly pleased to take part in the RECOVERY trial. I feel very lucky that the trial was underway when I was taken to the hospital with COVID-19 and was able to receive this innovative treatment. I’m happy that by participating, I played a part in finding this treatment successful."
Preliminary results from this evaluation of the monoclonal antibody combination will be available as a preprint on medRxiv and will be submitted to a leading peer-reviewed medical journal.
Professor Fiona Watt , chief executive of the Medical Research Council, which helped fund the study, said: “The flagship RECOVERY trial once again leads the way in showing the importance of well-designed clinical trials in identifying life-saving treatments. This very important finding means that, for hospitalized COVID-19 patients who do not produce their own antibodies against the virus, treatment with drugs based on antibodies against the spike protein may reduce the risk of death and the time they spend at the hospital. "Patients who have produced their own antibodies against the virus do not benefit from the new treatment, which is also important information given the cost of the drugs."
Professor Nick Lemoine , medical director of the NIHR Clinical Research Network, said: “It is fantastic news that the RECOVERY trial has provided evidence to establish another life-saving treatment for COVID-19 through this combination of antiviral antibodies. monoclonal. The incredible impact that the trial continues to have is a testament to the scientists and healthcare professionals, but equally to the tens of thousands of patients who have participated. "We want to sincerely thank each of them for their contribution."















