
Elevated levels of lipoprotein (a), a variant of ’bad cholesterol’ , in the bloodstream are a risk factor for recurrent coronary heart disease (CHD) in people aged 60 and older, according to the results of a new study that analyzed the problem over the course of 16 years.
The results, published in Current Medical Research & Opinion , suggest that current cholesterol-lowering medications may not be effective in reducing the risk of recurrent coronary heart disease, such as a heart attack, due to elevated Lp(a).
Future therapies to reduce elevated Lp(a) could help prevent recurrent disease
"This finding adds to the growing evidence of a relationship between increased Lp(a) and the risk of recurrent CHD," says senior author Associate Professor Leon Simons, of the New University School of Clinical Medicine. South Wales, Sydney. “It is well established that people who have already experienced CHD are at very high risk of suffering another event. Our new results indicate that new therapies in development that aim to reduce elevated Lp(a) levels could help prevent recurrent disease. However, the potential clinical benefit of the therapy in reducing elevated Lp(a) levels remains to be confirmed.”
Coronary heart disease is the most common type of heart disease. It occurs when the arteries that supply oxygen-rich blood to the heart narrow due to the buildup of fatty material within their walls. It is the most common cause of heart attack and was the leading cause of death for men and women worldwide in 2019.
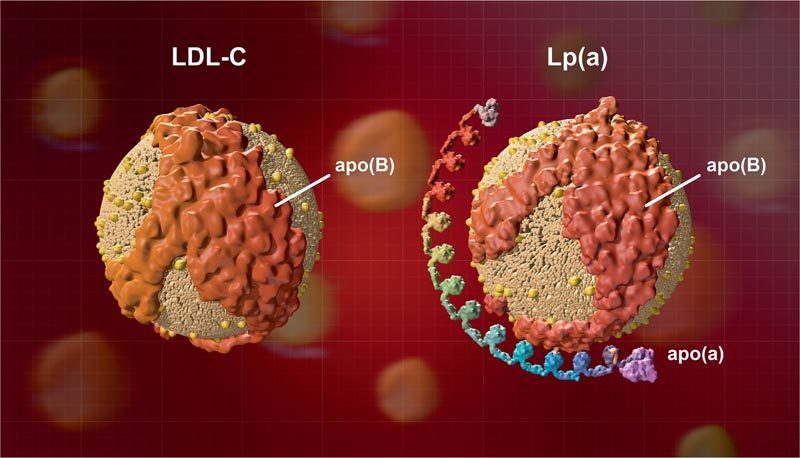
High blood cholesterol levels can increase the risk of coronary heart disease. Cholesterol travels through the blood in lipoproteins, which are made of proteins and fats. Lipoproteins include low-density lipoproteins (LDL), high-density lipoproteins (HDL), and Lp(a). LDL cholesterol is often called "bad cholesterol" because it builds up in the walls of blood vessels, increasing the chances of cardiovascular disease. Lifestyle changes and/or medications, such as statins, can help a person’s cholesterol levels stay within the healthy range.
While previous research has indicated that high Lp(a) levels are also an important risk factor in the development of CHD, most of these studies have looked at Lp(a) levels and the risk of a first CHD event. CHD. The current study examined whether elevated Lp(a) is predictive of a second or recurrent CHD event. It involved 607 Australians aged 60 and over, all with prevalent CHD, who were followed for 16 years as part of the Dubbo study. There were 399 incident cases of coronary heart disease.
The researchers found that:
|
In elderly people with prior CHD, elevated Lp(a) in the top 20% of the population distribution (>355 mg/L) predicted a 53% excess risk of a recurrent CHD event , compared with those in the bottom 20% of the population distribution (<50 mg/L) over 16 years of follow-up. This prediction was independent of other risk factors.
“We conclude that elevated Lp(a) is an important predictor of recurrent coronary heart disease in older people. “Upper baseline Lp(a) levels of 500 mg/L or 300 mg/L appear to be appropriate for identifying those at higher risk who may benefit from more intensive risk reduction interventions,” says Associate Professor Simons. “While current medications, such as statins, are often prescribed to reduce ’bad cholesterol’ in patients at higher risk of cardiovascular disease, they do not have any significant or proven impact on elevated Lp(a). But there is hope for the future, as some novel therapies that are designed to reduce Lp(a) levels are currently in advanced stages of clinical development.”
A key limitation of this longitudinal study is that the baseline data were collected in 1988-1989. However, although there may be other influences affecting the risk of CHD during the years of follow-up, especially with the use of statin therapy, it can be reasonably assumed that people with elevated Lp(a) levels at the start of the study They will maintain that state throughout the period.
Final synthesis Lipoprotein(a) [Lp(a)], a type of "bad cholesterol" , has been shown to be a major cause of coronary artery disease (CAD). In the long-term Dubbo Study of older people in Australia, Professor Simons’ team previously showed that citizens with Lp(a) readings above 276 mg/L were 46% more likely to suffer a first CAD problem (e.g., heart attack) compared to those who have much lower readings. This new study asked whether Lp(a) could also increase the chance of a second or repeat episode of DKA in citizens who had already developed DKA. In 607 older people with previous CAD followed for 16 years, those with Lp(a) readings greater than 355 mg/L were 53% more likely to develop another CAD problem compared to those with much lower readings. The team concluded that Lp(a) remains an important cause of recurrence of DKA in older people. The benefit of emerging treatments to lower Lp(a) remains to be confirmed in ongoing research. |















