Background
Elevated coronary artery calcium (CAC) scores in subjects without prior atherosclerotic cardiovascular disease (ASCVD) have been shown to be associated with increased cardiovascular risk.
Goals
The authors sought to determine at what level individuals with elevated CAC scores who have not had a prior atherosclerotic cardiovascular disease (ASCVD) event should be treated as aggressively for cardiovascular risk factors as patients who have already survived an ASCVD event.
Methods
The authors conducted a cohort study that compared event rates in patients with established prior atherosclerotic cardiovascular disease (ASCVD) with event rates in people with no history of ASCVD and known calcium scores to determine at what level elevated CAC scores are equivalent to the risk associated with existing ASCVD.
In the multinational CONFIRM registry ( Coronary CT Angiography Evaluation for Clinical Outcomes: An International Multicenter ), the authors compared ASCVD event rates in people without a history of myocardial infarction (MI) or revascularization (as classified by CAC scores). with event rates in those with established ASCVD.
They identified 4,511 individuals without known coronary artery disease (CAC) who were compared with 438 people with established ASCVD. Coronary artery calcium (CAC) scores were classified as 0, 1 to 100, 101 to 300, and >300.
Cumulative major adverse cardiovascular events ( MACE), MACE plus late revascularization, MI, and incidence of all-cause mortality were assessed using the Kaplan-Meier method for persons without a history of ASCVD by CAC level and persons with established ASCVD. Cox proportional hazards regression analysis was used to calculate HRs with 95% CIs, which were adjusted for traditional cardiovascular risk factors.
Results
The mean age was 57.6 ± 12.4 years (56% men). In total, 442 of 4,949 (9%) patients experienced MACE during a median follow-up of 4 years (IQR: 1.7-5.7 years). Incident MACE increased with higher CAC scores, with the highest rates observed with a CAC score > 300 and in those with prior ASCVD .
All-cause mortality , MACE, MACE + late revascularization, and MI event rates were not statistically significantly different in those with CAC > 300 compared with established ASCVD (all P > 0.05) .
People with a CAC score <300 had substantially lower event rates .
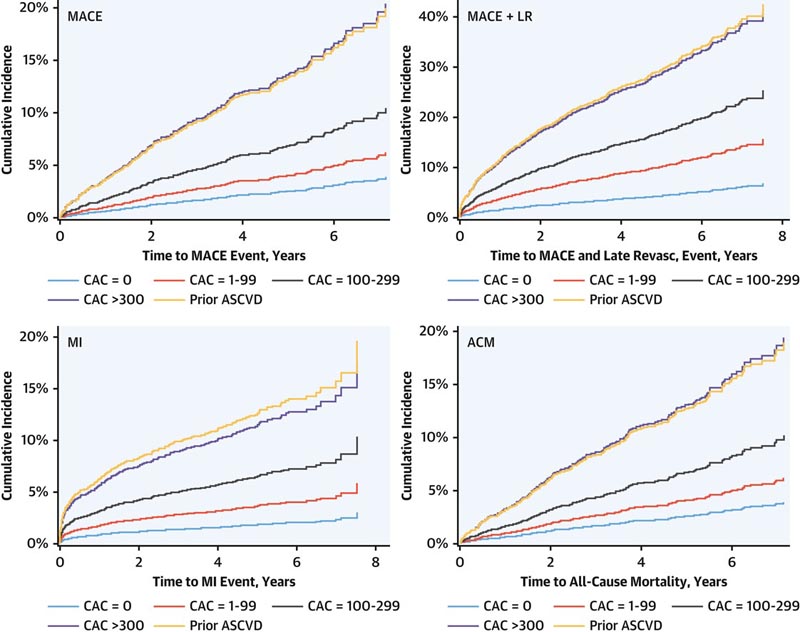
Conclusions Patients with CAC scores >300 have an equivalent risk of MACE and its components as those treated for established ASCVD. This observation, that those with CAC > 300 have comparable event rates to those with established ASCVD, provides important background for additional studies related to the goals of secondary prevention treatment in subjects without prior ASCVD with elevated CAC. Understanding CAC scores that are associated with ASCVD risk equivalent to stable secondary prevention populations may be important for guiding the intensity of preventive approaches more broadly. |















