
Participation in home-based cardiac rehabilitation was linked to a lower risk of death among veterans over a four-year follow-up, according to a new study published in the Journal of the American Heart Association .
Research Highlights:
|
Participating in home cardiac rehabilitation after a heart attack or cardiac procedure was associated with a 36% lower likelihood of death from heart-related complications among U.S. military veterans within four years compared to those who chose not to participate. rehabilitation programs, according to new research published today in the Journal of the American Heart Association , a peer-reviewed, open-access journal of the American Heart Association.
While cardiac rehabilitation has been shown to reduce the risks of hospital readmissions and death, according to the American Heart Association, it is significantly underutilized. Cardiac rehabilitation emphasizes eliminating tobacco use, improving diet, exercising, managing stress, and taking medications to treat high blood pressure or high cholesterol.
"Whether in a hospital or at home, cardiac rehabilitation is about healthy behavior changes," said study lead author Mary A. Whooley, MD, a primary care physician at the Veterans Affairs Medical Center ( VA) of San Francisco and professor of medicine at the University of California, San Francisco. “However, changing behaviors is difficult, and while care facilities can offer on-site cardiac rehabilitation, many patients do not choose to take advantage of follow-up treatment. “The biggest surprise from our analysis was how few patients chose to participate in cardiac rehabilitation.”
While cost may be a barrier to participating in cardiac rehabilitation, along with geography and logistics, cost should not have been a factor since healthcare services were covered by the VA in this study.
“We don’t know why so many patients opted out of rehabilitation,” Whooley said. “Even when home cardiac rehabilitation was offered at a time and place of their choosing, only 44% of eligible patients chose to participate. “Many patients were simply not interested in changing their behaviors.”
The data indicated that among patients hospitalized for a heart attack between 2007 and 2011, only 16% of Medicare patients and 10% of veterans participated in cardiac rehabilitation. Among eligible Medicare beneficiaries in 2016, only 24% chose to participate in on-site or facility-based cardiac rehabilitation. According to the Million Hearts® Cardiac Rehabilitation Collaborative , a national initiative co-led by the Centers for Disease Control and Prevention and the Centers for Medicare & Medicaid Services, increasing participation in cardiac rehabilitation to 70% of cardiac patients after of hospitalization could save 25,000 lives and prevent 180,000 additional hospitalizations each year.
“Many randomized trials have demonstrated similar mortality benefits of home and in-center cardiac rehabilitation,” Whooley said.
This is the first U.S. study to provide evidence of a survival benefit with home cardiac rehabilitation in people with heart disease, according to the study authors. The ongoing COVID-19 pandemic that temporarily closed countless facility-based rehabilitation programs indicates a growing need to explore opportunities in telehealth care for people with heart disease, they said.
This study analyzed data from 1,120 veterans who were eligible for cardiac rehabilitation at the San Francisco VA Medical Center between August 2013 and December 2018. Among this study group, 98% were men, 2% were women, 76 % were white, 88% were non-Hispanic, and 68% lived in an urban area. About half had been hospitalized for percutaneous coronary intervention, also known as angioplasty, 20% for a coronary artery bypass graft, 14% for a heart attack and 18% for other reasons. Enrollment in the San Francisco Healthy Heart home cardiac rehabilitation program was voluntary and only 44% (490 people) enrolled.
The at-home cardiac rehabilitation program lasted 12 weeks, during which participants received up to nine counseling calls, motivational interviews, a workbook, and a personal health diary to document vital signs, exercise, and diet. They also received a blood pressure monitor, a scale and (if they wanted) a stationary bicycle. A nurse worked individually with participants to create achievable physical activity goals. Participants received follow-up telephone calls from program staff three and six months after program completion and were followed for an average of 4.2 years after hospitalization.
Among the researchers’ findings:
- The mortality rate one year after hospitalization was 4% among those who did not participate in cardiac rehabilitation versus 2% among those who participated in home cardiac rehabilitation.
- Overall, those who participated in the cardiac rehabilitation program were associated with a 36% reduction in the odds of dying from complications compared to those who did not.
- Deaths occurred throughout the follow-up period in 12% of rehabilitation participants versus 20% of non-participants.
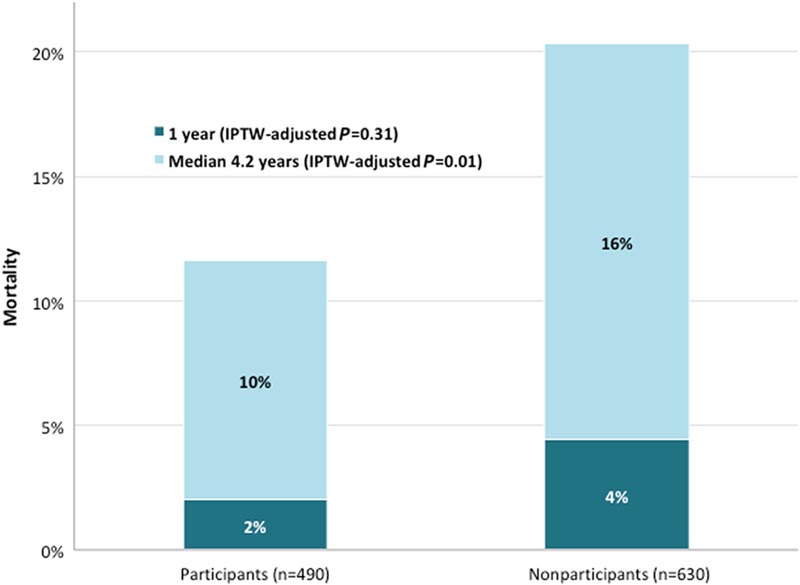
Figure : Mortality in home cardiac rehabilitation participants versus nonparticipants with inverse probability of treatment weighted P values.IPTW indicates the inverse probability of treatment weighting .
The researchers note that scientists do not yet know the optimal number of home cardiac rehabilitation sessions needed to achieve lasting success for people with heart disease, and this warrants further research. Additionally, compared to traditional facility-based programs, researchers believe that home-based cardiac rehabilitation may lead to longer-lasting behavioral changes that improve outcomes, because integrating healthy behaviors into a participant’s home routine from The principle has been associated with improved compliance rates.
While there is no standardized approach to providing cardiac rehabilitation at home, it is typically shorter than on-site care and "as technology expands, behavior modification in participants’ home environment can help make cardiac rehabilitation more accessible and lifestyle changes more accessible," Whooley said.
Another advantage of at-home cardiac rehab is that, because capacity is not limited by the availability of on-site programs, wait times to begin therapy are shorter (an average of 25 days versus 77 days later). of a cardiac event).
“Our biggest challenge in the U.S. is that many health insurers do not cover home cardiac rehabilitation,” he said. “Currently, Medicare only pays for on-site or facility-based cardiac rehab.”
The American Heart Association supports congressional legislation, such as the bipartisan “Increasing Access to Quality Cardiac Rehabilitation Care Act,” that calls for the expansion of cardiac rehabilitation resources.
Randal J. Thomas, MD, chair of the 2019 American Heart Association and American College of Cardiology Joint Statement on the Effectiveness of Home Cardiac Rehabilitation, called this study a " unique landmark report . "
"This study suggests that home cardiac rehabilitation is associated with a lower mortality rate compared to people who do not receive cardiac rehabilitation," said Thomas, a professor of medicine at Mayo Clinic’s Alix School of Medicine who works with Mayo Clinic Cardiac Rehabilitation Program in Rochester, Minnesota. “Previous studies of home cardiac rehabilitation have not been designed to address this important benefit. Additional studies are needed, but this study strongly suggests a mortality benefit from home cardiac rehabilitation."
“Although the study did not clarify whether home cardiac rehabilitation affects mortality rates as well or even better than in-center rehabilitation, it does show that home cardiac rehabilitation reduces mortality rates compared to those patients who do not participate in rehabilitation cardiac. "
The joint statement strongly recommends cardiac rehabilitation for people diagnosed with a heart attack, chest pain, heart failure, or after undergoing bypass surgery, percutaneous coronary intervention, heart valve surgery, or a heart transplant. Additionally, a scientific statement from the American Heart Association notes that home rehabilitation is an effective alternative to cardiac rehabilitation for those who cannot participate in an on-site cardiac rehabilitation program.
The study has several limitations , including that there was no comparison with in-center cardiac rehabilitation; participants were not randomly assigned; and most were older men who spoke English. The researchers note that it is unclear whether the benefits of home-based cardiac rehabilitation would produce similar benefits in women or non-English speakers.
Clinical Perspective What’s new? This observational study provides pragmatic evidence of survival benefit with home cardiac rehabilitation in patients with cardiac disease. What are the clinical implications? Patients who underwent home cardiac rehabilitation had a 36% lower risk of mortality after a median of 4.2 years of follow-up. Our study findings indicate that home-based cardiac rehabilitation may benefit eligible patients who are unable to attend traditional cardiac rehabilitation programs. |
Co-authors are Nirupama Krishnamurthi, MBBS, MPH; David W Schopfer, MD MAS; Hui Shen, M.Sc.; Gregory Rohrbach, DNP; and Abdelaziz Elnaggar, MBBS, MPH Author disclosures are listed in the manuscript.















