Sudden cardiac death ( SCD) in young competitive athletes is caused by a broad spectrum of cardiovascular conditions, including congenital heart disease, genetic cardiomyopathies and channelopathies, and acquired conditions. Cardiovascular evaluation of athletes prior to participation in competitive sports offers the potential to identify athletes with cardiovascular disease at risk for SCD and prevent sports-related deaths. The American Heart Association (AHA), the European Society of Cardiology (ESC), the International Olympic Committee, and most medical associations and sports federations around the world recommend preparticipation screening (PPS). However, the optimal PPS protocol is still debated with particular reference to the inclusion of a screening electrocardiogram (ECG), the appropriate age of onset and frequency of repeat cardiovascular evaluations, and the eligibility of athletes diagnosed with at-risk cardiovascular diseases. from MSC.
An outcome study in English soccer players who underwent a single session of PPS that included a single assessment at the age of 16 years reported an incidence of SCD during long-term follow-up much higher than historical estimates. Unlike this screening modality, the Italian program, which has been in practice since 1982, requires that preparticipation cardiovascular evaluation, including ECG, begin at the beginning of sporting activity (even in early childhood) be repeated every year and implies the ineligibility for competitive sports activity of athletes diagnosed with cardiovascular disease at risk of SCD.
Goals
This study aimed to report the long-term findings of the Italian pre-participation cardiovascular screening (PPS) program in young, competitive athletes.
The present study was designed to evaluate the results of the Italian PPS program in a large population of children (7 to 18 years of age), evaluating the diagnostic performance of cardiac diseases with risk of SCD, the costs of serial cardiovascular evaluations and the long-term result.
Methods and results
The study evaluated the diagnostic performance of diseases with risk of sudden cardiac death (SCD), the costs of serial evaluations, and the long-term outcomes of SPP in a large population of Italian children (age range, 7 to 18 years ). The PPS was repeated annually and included medical history, physical examination, resting electrocardiogram, and stress testing; Additional testing was reserved for athletes with abnormal findings .
During an 11-year study period , 22,324 consecutive children [62% male; median age, 12 (interquartile range, 10-14) years at first screening] underwent a total of 65,397 annual evaluations (median, 2.9/child).
Cardiovascular diseases with risk of SCD were identified in 69 children (0.3%) and included congenital heart diseases (n = 17), channelopathies (n = 14), cardiomyopathies (n = 15), non-ischemic left ventricular scar with ventricular arrhythmias ( n = 18) and others (n = 5).
Risk cardiovascular diseases were identified across the entire age range and most frequently in children ≥12 years (n = 63, 91%) and at repeat evaluation (n = 44, 64%). The estimated cost per diagnosis was €73,312.
During a follow-up of 7.5 ± 3.7 years, one child with normal PPS results experienced an episode of resuscitated cardiac arrest during sports activity (event rate 0.6/100,000 athletes/year).
Conclusion
The PPS program led to the identification of cardiovascular diseases at risk for SCD across the entire age range of study children and more often in repeated assessments. Among children evaluated, the incidence of sports-related cardiac arrest during long-term follow-up was low .
Structured graphic summary
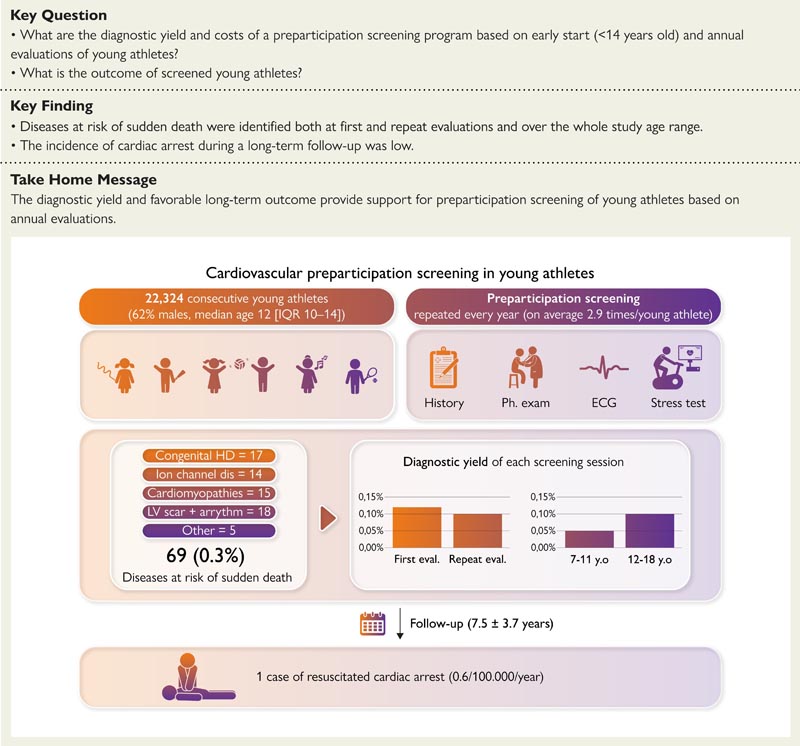
The study enrolled a cohort of 22,324 children who underwent an average of 2.9 annual preparticipation examinations that included history, physical examination, resting ECG, and exercise testing. Cardiovascular diseases with risk of sudden cardiac death were identified in 69 children (0.3%). The diagnostic yield of each screening session was 0.12% at the first assessment and 0.1% at the repeat assessment. Furthermore, it was 0.05% in children aged 7 to 11 years compared to 0.12% in those aged 12 to 18 years. During a follow-up of 7.5 ± 3.7 years, one child with normal preparticipation screening results experienced an episode of resuscitated cardiac arrest during sports activity. HD, heart disease; VI, left ventricle; IQR, interquartile range .
Discussion
The present study was designed to evaluate the results of annual cardiovascular PPS in a large cohort of Italian children (age range, 7-18 years). The main results of the study were that (i) the overall diagnostic yield of cardiovascular diseases, whether associated or not associated with SCD, among asymptomatic children was 1.8% across a mean of three PPS assessments; (ii) the identification of cardiovascular diseases associated with SCD covered the entire study age range of children with a trend towards increasing diagnostic performance with increasing age; (iii) The diagnostic performance of repeated (annually) screening assessments was similar to that of the first screening, representing an increase in overall diagnostic performance of almost two-thirds compared to a single screening.
Final message The PPS program led to a diagnosis of cardiovascular disease with risk of SCD across the entire age range of study children and was associated with a low incidence of life-threatening cardiovascular events. The probability of identifying a risk condition was similar between repeat screening and the first screening session, representing an increase in overall diagnostic performance of almost two-thirds compared to single screening. The favorable long-term outcome and survival provide additional support to the value of early detection through PPS and appropriate management of cardiovascular diseases at risk for SCD in the childhood population. |















