
Highlights
|
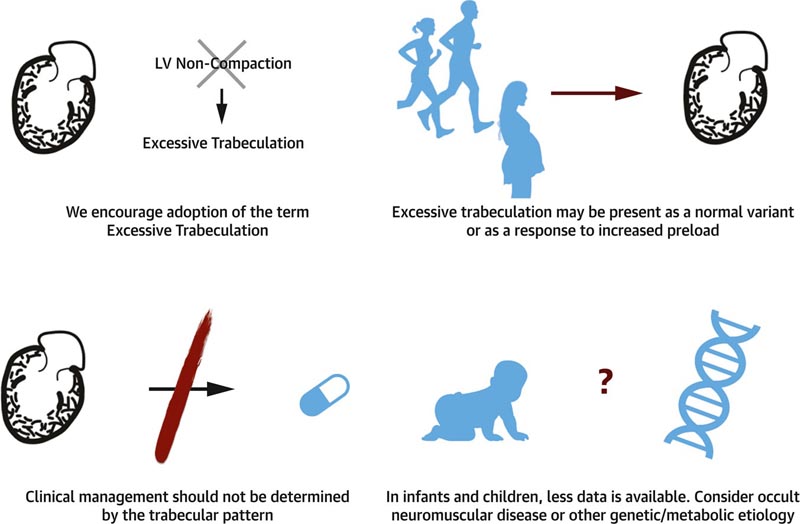
Excessive trabeculation is a ventricular phenotype identified by imaging studies, most commonly echocardiography and cardiac magnetic resonance (CMR). Like the thickness or diameter of the ventricular wall, the presence of excessive trabeculation alone does not define the presence of cardiomyopathy. As noted by Jenni, Oechslin, and colleagues, excessive trabeculation may be a normal variant or a physiological response to conditions of increased preload or afterload, such as pregnancy or athletic participation.
Because of considerable variation in the extent of ventricular trabeculation in the population, individuals with excessive trabeculation in isolation may pose diagnostic and treatment challenges. For example, excessive trabeculation is reported to be associated with some pathological conditions , including well-recognized cardiac muscle disorders. In such cases, it is often unclear whether the phenotype itself identifies a very specific (and rare) cardiomyopathy (i.e., so-called left ventricular noncompaction cardiomyopathy ) or represents a secondary response to altered preload and/or afterload. in patients with myocardial dysfunction.
In this expert consensus document, we summarize published reports related to excessive trabeculation and its association with cardiomyopathy in both children and adults. Except for historical context, we avoid the term “noncompaction” because new developmental biology research shows that the term misrepresents the nature of fetal ventricular wall development. We use the term “excessive trabeculation” when left ventricular trabecular morphology exceeds previously described thresholds. Additionally, we offer considerations for managing patients in a variety of situations with excessive trabeculation.
Summary
Excessive trabeculation, often referred to as “uncompacted” myocardium, has been described in all ages, from fetus to adult. However, current evidence on myocardial development does not support the formation of compact myocardium from non-compacted myocardium, nor the arrest of this process to give rise to so-called non-compaction. Excessive trabeculation is frequently observed by imaging studies in healthy individuals, as well as in association with pregnancy, sports activity, and with cardiac diseases of inherited, acquired, developmental, or congenital origin. Adults with incidentally noted excessive trabeculation often do not require further follow-up based on trabecular pattern alone.
Patients with cardiomyopathy and excessive trabeculation are treated for cardiovascular symptoms rather than the trabecular pattern. To date, the prognostic role of excessive trabeculation in adults has not been shown to be independent of other myocardial diseases. In neonates and children with excessive trabeculation and normal or abnormal function, clinical caution appears warranted due to the reported association with genetic and neuromuscular disorders. This report summarizes the evidence on the etiology, pathophysiology and clinical relevance of excessive trabeculation. Gaps in current knowledge of the clinical relevance of excessive trabeculation are indicated, and priorities for future research and improved diagnosis in adults and children are suggested.
Definitions of excessive trabeculation
Several quantitative definitions for excessive trabeculation have been proposed. Most commonly, echocardiographers use the criteria published by Jenni et al. These include, first, the presence of a 2-layer myocardium; second, a trabecular-to-compact myocardium ratio >2:1 measured at end-systole in the short-axis view. The typical location of the most pronounced trabeculation in the mediolateral, apical, and medioinferior segments and the absence of coexisting cardiac anomalies are presumed . In a recent meta-analysis seeking to evaluate the prevalence of so-called noncompaction, almost two-thirds of published echocardiographic studies used criteria that included trabecular to compact myocardium >2:1 at end-systole. Using this reference, the prevalence among 23 cohorts was 0.56%. To our knowledge, the prevalence of excessive trabeculation, 0.076%, was assessed in only 1 population-based neonatal echocardiographic study.
Excessive trabeculation as measured by current criteria occurs in individuals without cardiomyopathy . When applied to the general population, Petersen criteria were met in approximately 20% of participants in 5 population-representative cohorts in at least 1 myocardial segment. Therefore, researchers have also considered parameters such as the relative or absolute thickness and mass of the trabecular and compact layers, the number of affected segments, the location of affected segments, trabecular morphology, and papillary muscle morphology.
It is also possible that conventional descriptors are too simplistic to capture our visual impression of excessive trabeculation. The fractal dimension of CMR is an example of a sophisticated and highly reproducible mathematical score of endocardial complexity ranging from 1 (a straight line) to 2 (complete filling of the two-dimensional space contained by ventricular trabeculation).
Associations with neuromuscular diseases
Excessive trabeculation has been observed in several neuromuscular disorders , including specific genetically determined conditions such as Barth syndrome, mitochondrial disorders, nuclear envelopes, dystrobrevinopathy, myotonic dystrophy, zaspopathy, and myoadenylate deaminase deficiency, as well as Duchenne and Becker which are types of muscular dystrophy. However, a causal relationship with the underlying genetic defects has not yet been established, and the genotypic-phenotypic heterogeneity remains largely unexplained. The combination of phenotype and neuromuscular disease, however, may have clinical and prognostic implications.
The pregnancy
Reversible excessive trabeculation is known to develop secondary to increased preload in a considerable proportion of pregnant women with otherwise normal hearts . The feature had generally resolved by 12 weeks postpartum, although with some variability in regression of the trabecular layer, similar to the variation in reduction in overall left ventricular mass. African American women were 3 times more likely to develop such characteristics during pregnancy than Caucasian women. This suggests a possible genetic susceptibility underlying the adaptive response of the myocardium to volume and pressure overload.
Exercise
A reversible phenotype of excessive trabeculation has been reported in athletes. This is recognized as a morphological epiphenomenon related to the high cardiac preload demand associated with intensive physical exercise. The prevalence of ratios meeting the criteria for excessive trabeculation among competitive athletes by echocardiography ranges between 1.4% and 8.1%. This varies depending on different definitions, ethnicities, and specific sports disciplines.
Conclusions
This review summarizes the evidence and uncertainties regarding the phenotypic characteristic of excessive trabeculation and its potential associations with cardiomyopathies (Central Illustration). Because the trabeculated myocardium does not fuse to form the compact myocardial wall, the traditional terminology of left ventricular noncompaction should be discouraged. Excessive trabeculation is frequently detected in the presence of features of a cardiac muscle disorder, but is also frequently found as a normal variation or develops as a reversible component of physiological cardiac adaptation.
Recognition of a highly trabeculated left ventricle is not known to influence prognosis or treatment in adults. In newborns and children, caution is warranted because there are multiple reports with genetic abnormalities and neuromuscular disorders in this vulnerable population. Future efforts are warranted to characterize the outcomes and characteristics of those presenting with excessive trabeculation.
* Access to the complete report in English .
Comments
The main pumping chamber of the heart, the lower left ventricle, contains pieces of muscle called trabeculations that extend into it. Excessive trabeculation, often referred to as uncompacted myocardium, has been described in all ages, from fetus to adult.
Numerous previous studies have reported excessive trabeculation in healthy individuals, possibly due to the influence of changes in circulatory load such as pregnancy or exercise, in coexistence with well-known heart muscle diseases such as dilated cardiomyopathy or hypertrophic cardiomyopathy, or in relation to with a rare entity called non-compaction cardiomyopathy.
The review article and expert consensus document are published in the leading cardiac imaging journal, JACC Cardiovascular Imaging , and are led by world experts in heart muscle diseases and cardiovascular imaging, from the William Harvey Research Institute at Queen’s University. Mary of London and the NIHR Barts Biomedical Research Centre.
Among its highlights, the document warns that since the trabeculated cardiac muscle does not coalesce to form the compact myocardial wall, the term ’left ventricular noncompaction cardiomyopathy’ , which prevails in contemporary medical literature, is inaccurate , so its use should be discouraged.
Senior author Steffen E. Petersen, professor of cardiovascular medicine at Queen Mary and honorary consultant cardiologist at Barts Health NHS Trust, says:
“We anticipate that the scientific community will move away from the term ’LV noncompaction ,’ which is misleading, to use ’excessive trabeculation,’ which can be observed in a wide spectrum of health states and diseases.
“The recommendation of this work has substantial clinical impact as it can reduce harm to patients and people often mislabeled as carriers of a specific disease. "We also hope that this review article and expert consensus will lead to further research to better characterize the genetic basis and physiological impact of excessive trabeculation in otherwise normal individuals."
Co-author Dr Nay Aung, academic clinical professor at the National Institute for Health and Care Research (NIHR) at Queen Mary and cardiologist, adds:
“Based on the available evidence, this expert consensus provides pragmatic recommendations on the clinical management of adults with incidental excessive trabeculation and those diagnosed with hypertrophic or dilated cardiomyopathy along with excessive trabeculation. The evidence is relatively scarce in children with excessive trabeculation, so this population may follow a different clinical trajectory, hence the need for further research.”
The experts summarized the evidence and uncertainties about the characteristics of excessive trabeculation and its possible associations with cardiomyopathies, diseases of the heart muscle that make it more difficult to pump blood throughout the body.















