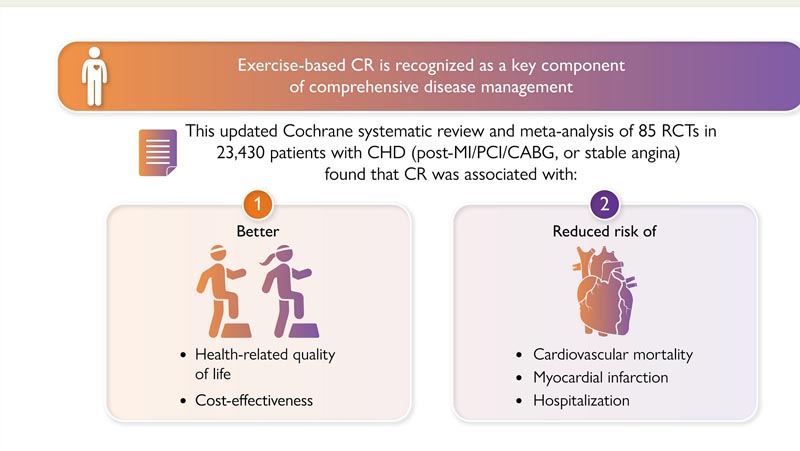
Coronary heart disease (CHD) is the most common cause of death worldwide. With increasing numbers of people living longer with CHD, accessible and effective health services for the management of CHD are crucial. Exercise-based cardiac rehabilitation ( CR) is recognized as a key component of comprehensive CHD management and is a Class I Grade A recommendation in international guidelines.
Although meta-analyses of randomized controlled trials (RCTs) have demonstrated the beneficial effect of CR in patients with CHD, this evidence base has been questioned on the grounds of: (i) uncertainty in the impact on mortality; (ii) lack of data on health-related quality of life (HRQoL); (iii) the inclusion of RCTs limited to low-risk patients and conducted in high-income country settings, and (iv) the lack of trials conducted during the era of modern CHD therapy.
To address these uncertainties, we conducted a contemporary update of the Cochrane systematic review and meta-analysis of RCTs to evaluate the effects of exercise-based CR in patients with CHD on mortality, clinical events, HRQoL, and cost-effectiveness. We also sought to explore whether intervention effects varied with patient case mix, study and intervention characteristics, and CR delivery settings.
Goals
Coronary heart disease is the most common reason for referral to exercise-based cardiac rehabilitation (CR) worldwide. However, the generalizability of previous meta-analyses of randomized controlled trials (RCTs) is questioned. Therefore, a contemporary updated meta-analysis was performed.
Methods and results
We searched databases and trial registries up to September 2020 for RCTs of exercise-based interventions with follow-up of ≥6 months, compared with non-exercise control for adults with myocardial infarction, angina pectoris or after coronary artery bypass grafting, or percutaneous coronary intervention.
Mortality, recurrent clinical events, and health-related quality of life (HRQoL) outcomes were pooled using a random-effects meta-analysis and cost-effectiveness data were narratively synthesized. Meta-regression was used to examine effect modification. Study quality was assessed using the Cochrane risk of bias tool. A total of 85 RCTs were included with 23,430 participants with a median follow-up of 12 months.
- Overall, exercise-based CR was associated with significant risk reductions in cardiovascular mortality [relative risk (RR): 0.74, 95% confidence interval (CI): 0.64–0.86, number needed to treat (NNT): 37], hospitalizations (RR: 0.77, 95% CI: 0.67–0.89, NNT: 37), and myocardial infarction (RR: 0.82, 95% CI: 0 .70–0.96, NNT: 100).
- There was some evidence of significant improvement in health-related quality of life (HRQoL) with CR participation, and CR is cost-effective.
- There was no significant impact on overall mortality (RR: 0.96, 95% CI: 0.89–1.04), coronary artery bypass grafting (RR: 0.96, 95% CI: 0.80–1.04), 1.15) or percutaneous coronary intervention (RR: 0.84, 95% CI: 0.69-1.02).
- No significant differences in effects were found between different patient groups, CR delivery models, dosing, follow-up, or risk of bias.
Conclusion
This review confirms that participation in exercise-based CR by patients with coronary heart disease receiving contemporary medical treatment reduces cardiovascular mortality, recurrent cardiac events and hospitalizations and provides additional evidence supporting improvements in quality of life related to health (HRQoL) and the profitability of CR.
Discussion
This updated Cochrane review and meta-analysis of RCTs incorporated data from >23,000 patients with CHD and confirmed the benefits of participation in exercise-based CR including reductions in the risk of cardiovascular mortality, myocardial infarction, and all-cause hospitalization in a median follow-up up to 12 months. No significant differences in effect were found between patient case mix, type or set of CR program, prescribed exercise dose, study sample size, location, duration of follow-up, year of publication and the ROB. Reducing hospitalizations is likely to have benefits for both healthcare services and patients in terms of health resource use and associated costs, and an early return home to families and community support networks.
Importantly, this updated review demonstrates that the benefits of CR extend through recent trials that are more representative of the modern therapeutic approach in CHD, the expanded CHD population, and low- and middle-income settings (21 trials conducted in LMIC with 7851 participants), where the prevalence of coronary heart disease continues to increase.
CHD is clinically shifting from a life-threatening disease to a chronic disease trajectory , as reflected in the terminology of current clinical guidelines on chronic coronary syndromes. This crucial change strongly calls for interventions that contribute to improving the rehospitalization rate, well-being, and HRQoL of people living with chronic diseases. Therefore, this latest Cochrane review of RCTs still reinforces the importance of exercise-based CR as part of integrated CHD care along with modern invasive and pharmacological therapy.
Final message The findings of this latest Cochrane review of 85 RCTs in 23,430 CHD patients confirm the clinical outcome benefits of reduced CV mortality, MI, and hospitalization with participation in exercise-based CR and also provide timely evidence supporting the generalizability of these. benefits among patients, in the context of contemporary medical management and in all healthcare settings, including LMICs. This updated review also provides meta-analytic evidence that participation in CR improves patient quality of life based on validated HRQoL data. Our findings reinforce the need to improve access to CR for patients with CHD worldwide. |















