Ventricular fibrillation and sudden death caused by a blunt, blunt, and often innocent-looking blow to the chest, without damage to the ribs, sternum, or heart (and in the absence of underlying cardiovascular disease) constitute an event known as commotio cordis , which translates from Latin as stirring of the heart. This term was first used in the 19th century, 1-6 although the appearance of commotio cordis was described earlier, in accounts of the ancient Chinese martial art of Dim Mak (or touch of death), in which the left of the sternum caused sudden death in opponents.
The absence of structural cardiac injury distinguishes commotio cordis from cardiac contusion, in which high-impact blows cause traumatic damage to the myocardial tissue and overlying chest.
Beginning in the mid-1700s, sporadic accounts of commotio cordis appeared in medical literature, primarily in the context of workplace accidents, and until the mid-1990s, the disorder was only occasionally noted in case reports, and largely went unnoticed except by the forensic pathology community and the Consumer Product Safety Commission. Since then, however, both the general public and the medical community have become increasingly aware of commotio cordis as a major cause of sudden cardiac death. It occurs primarily in children, adolescents, and young adults, most frequently during participation in certain recreational or competitive sports, with rare occurrences during normal, routine daily activities.
Continued interest in commotio cordis and its tragic consequences is evident in epidemiological studies and various experimental laboratory investigations. 20-35 This review focuses on the available information on the clinical profile, proposed mechanisms, and prevention and treatment of commotio cordis .
Incidence
- The precise incidence of commotio cordis is unknown due to the lack of systematic and mandatory reporting, but according to data from the National Commotio Cordis Registry in Minneapolis it is among the most common cardiovascular causes of sudden death in young athletes, after hypertrophic cardiomyopathy and congenital anomalies of the coronary arteries. Since commotio cordis occurs in a wide variety of circumstances, it has undoubtedly been underreported but is increasingly recognized and is probably more common than is believed.
- 95% of the cases affected men.
- Commotio cordis occurs most frequently in people aged 10 to 18 years, however, cases have been documented between 7 weeks and 51 years.
- 50% of episodes occur during competitive sports, another 25% occur during recreational sports, and the other 25% occur during other activities that involve blunt trauma to the chest wall, e.g., kicking a horse, acts of violence.
- Baseball has the highest incidence of commotio cordis , followed by softball, hockey, and then the football codes.
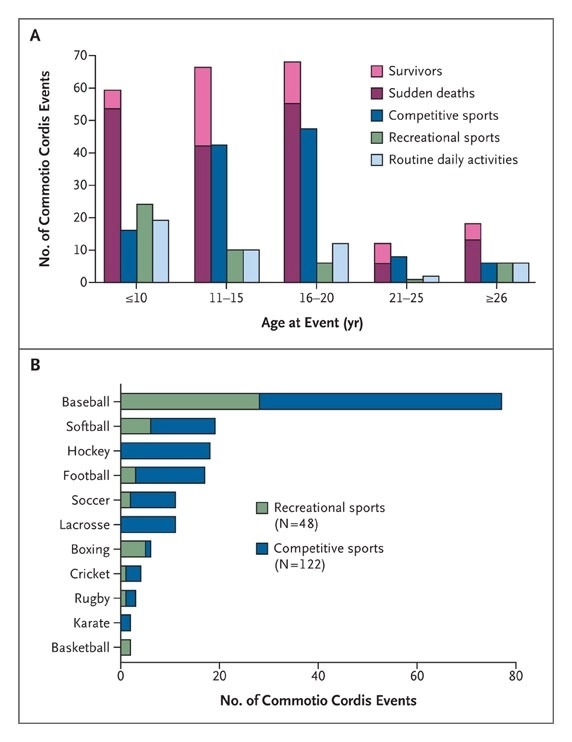
Figure : Distribution of Commotio Cordis events according to age and activity. Panel A shows the distribution of commotio cordis events by age and type of activity in 224 cases from the National Commotio Cordis Registry recorded in the last 15 years. Panel B shows the distribution of such events according to the particular sport.
About 50% of commotio cordis events have been reported in young competitive athletes (primarily between 11 and 20 years of age) participating in a variety of organized amateur sports, typically baseball, softball, ice hockey, soccer, or lacrosse, who receive a blow to the chest that is usually (but not always) delivered by a projectile used to play the game. In baseball, for example, it is often triggered when players are hit in the chest by balls that have been thrown, batted, or pitched in a variety of scenarios. In hockey, defensive players may intentionally use their chests to block the puck from an opponent’s high-speed shot. High school and college lacrosse players (including goalies with chest protectors) may be at greater risk for commotio cordis than athletes in other sports that involve similar solid projectiles (e.g., baseballs). Commotio cordis can also result from physical contact between competitors. Such blows to the chest are produced by the shoulder, forearm, elbow, leg, foot or head, as when two outfielders inadvertently collide while following a baseball in the air or, alternatively, when a hockey stick stabs into an opponent’s chest.
Another 25% of commotio cordis events occur in recreational sports played at home, on the playground, at picnics, or other family gatherings. These seemingly innocent events occur disproportionately in the youngest known victims (10 years or younger), with close family members (e.g., parents or siblings) or friends often responsible for the hit. In one example, a boy playing catch with one of his parents misjudged the flight of the ball, which then deflected off his glove and hit his chest. In recreational sports, the velocity of projectiles that cause chest hits varies widely, from low-speed balls thrown during informal games of catch to high-speed lacrosse or cricket.
Commotio cordis is not related to sports activities in approximately 25% of victims (most often younger ones). These incidents occur in a wide variety of circumstances, such as being kicked in the chest by a horse or hit by a playground swing when it bounces. Sometimes such accidents are brought to court. Charges of murder or manslaughter have led to criminal prosecution and imprisonment.
Commotio cordis is usually, but not invariably, fatal.
In only about 25% of cases reported in the Minneapolis registry did CPR or defibrillation result in survival, a low percentage considering that commotio cordis is defined by the absence of structural heart disease. The result is largely related to the circumstances under which the commotio cordis occurs . Fatalities have often been associated with the inability of bystanders to appreciate the life-threatening nature of the collapse and to initiate appropriately aggressive and timely resuscitative measures.
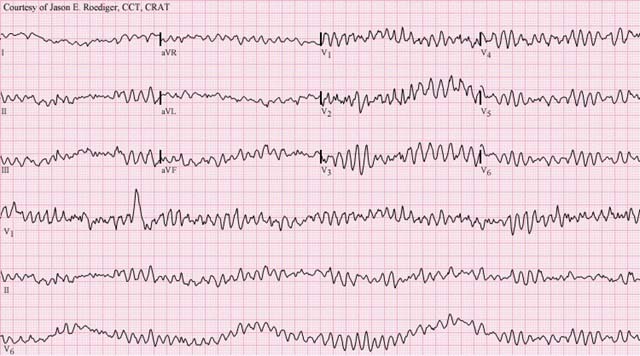
Registry data show that survival rates have increased over time, reaching 35% over the past decade, compared with 15% over the previous 10 years (P = 0.01); More recently, between 2006 and 2009, the number of successful resuscitations exceeded the number of deaths by 20%. This improvement is likely the result of increased public awareness, increased availability of automated external defibrillators (AEDs), and earlier activation of the chain of survival. Arrhythmias recorded at the time of collapse or in the emergency room are often caused by ventricular fibrillation, suggesting that restoration of sinus rhythm and survival are possible with rapid defibrillation. Some commotio cordis events may abort spontaneously, when the shock causes non-sustained arrhythmias, although this is difficult to confirm.
Commotio cordis is a primary arrhythmic event that occurs when the mechanical energy generated by a stroke is limited to a small area of the precordium and profoundly alters the electrical stability of the myocardium, resulting in ventricular fibrillation. A variety of biological and biomechanical experimental models have been developed to elucidate the mechanisms by which a rapid mechanical stimulus to the thorax triggers ventricular fibrillation. Early investigations yielded several theoretical explanations for the mechanics of the event, including excessive autonomic (vagal) reflex and coronary arterial vasospasm that have since been abandoned . During testing on later models, baseballs were propelled at speeds of up to 153 km (95 miles) per hour, resulting in serious injuries to the chest and heart (cardiac contusion), but no commotio cordis .
More recent experimental laboratory studies conducted under controlled conditions in pigs, dogs, and rabbits have provided insights into the underlying mechanisms of commotio cordis that are consistent with its clinical profile and have dispelled the notion that sudden death after a blow to the breast is a mysterious phenomenon. A model, in which projectile-induced shocks over a wide range of velocities were delivered to anesthetized young pigs in synchronization with the cardiac cycle, revealed two critically important mechanical determinants of ventricular fibrillation and lethality.
The first of these determinants involves the location of the blow , which must be directly over the heart (particularly at or near the center of the cardiac silhouette). This finding is consistent with clinical observations that precordial hematomas representing the imprint of a blow are frequently evident in victims. There is no evidence in humans or experimental models that sustained blows outside the precordium (e.g., the back, flank, or right side of the chest) cause sudden death.
The second determinant concerns the timing of the stroke , which must occur within a narrow window of 10 to 20 ms in the rise of the T wave , just before its peak (representing only 1% of the cardiac cycle), i.e. That is, the stroke must occur during an electrically vulnerable period , when the inhomogeneous dispersion of repolarization is greatest, creating a susceptible myocardial substrate for provoked ventricular fibrillation. In pigs, when shocks occurred outside of this brief time window, ventricular fibrillation was not the consequence; instead, what followed was transient complete heart block, left bundle branch block, or ST segment elevation. These effects have also been reported in some human survivors (with the presumed timing of the hit coinciding with the QRS complex during ventricular depolarization).
The impact energy associated with commotio cordis is not uniform, characteristically spanning a wide range of velocities as well as projectile sizes, shapes, and weights. Other factors that may increase the risk of ventricular fibrillation and commotio cordis include the hardness of the object and its size and shape, with hard, small, sphere-shaped projectiles more likely to cause damage.
The predisposition to commotio cordis in young people may be largely related to the physical characteristics of the chest in young people; the relatively thin, underdeveloped and compliant rib cage (and immature intercostal musculature) is less able to buffer the arrhythmogenic consequences of precordial shocks. Additionally, since children are likely to suffer chest blows more frequently than adults in a variety of circumstances, they may generally be at higher risk for concussion cordis .
Adults probably get a measure of protection from their mature, fully developed ribcage, which may partly explain the apparently low rate of commotio cordis events in sports such as kickboxing and boxing (accounting for less than 5% of cases). registered). In boxing, it is also possible that the glove itself, which increases the impact area, helps cushion the force of the blow.
The question of whether susceptibility to commotio cordis varies due to individual variations in QT interval duration has been considered but remains unanswered. There is no evidence that commotio cordis survivors are at increased risk of subsequent arrhythmic events, nor is there evidence that athletes who have had a commotio cordis event should be disqualified from competition for that reason alone. Similarly, prophylactic implantable defibrillators are not indicated for people who have survived shock cordis in the absence of cardiac disease.
Critical variables for the induction of ventricular fibrillation
The confluence of several critical variables is necessary to induce ventricular fibrillation with a balloon impact (Figure). If all currently known variables are maximized, approximately 30% of impacts at 30 mph and 50% of impacts at 40 mph will produce ventricular fibrillation in a 20 kg pig. Perhaps the most important variable is the timing of impact relative to the cardiac cycle (Figure). Only impacts in a narrow region on the upward slope of the T wave (40 ms before the peak of the T wave peak to the peak of the T wave) will cause ventricular fibrillation, with a markedly greater likelihood with impacts of 30 to 10 ms before the peak of the T wave.
Although polymorphic ventricular tachycardia was most frequently observed during impacts in these time periods, it was also occasionally induced by impacts at other times in the cardiac cycle. This polymorphic ventricular tachycardia was identical in morphology to the onset of ventricular fibrillation; however, it only continued up to 10 beats. If polymorphic ventricular tachycardia continued beyond 10 beats, it degenerated into ventricular fibrillation.
Heart block is rarely seen and is more common with smaller animals, with baseball impacts compared to lacrosse balls, and with greater impact velocity (unpublished data). Impacts throughout the cardiac cycle can cause ST segment elevation and left bundle branch block in those impacts in which ventricular fibrillation is not induced. Premature ventricular beats are almost always observed.
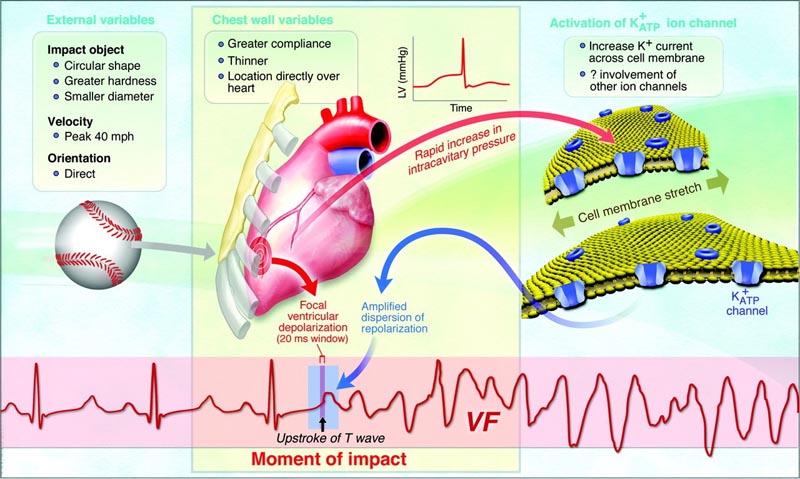
Figure : The confluence of variables and a proposed mechanism necessary for commotio cordis to occur. The important variables of the impact object are shape, hardness, diameter and speed. Human characteristics are the flexibility of the chest wall, the moment of impact, the location and orientation of the blow and individual susceptibility, probably carried in the ion channels involved in repolarization. LV indicates left ventricle. Reprinted from Journal of Cardiovascular Electrophysiology .
Source : Commotio Cordis. Ventricular Fibrillation Triggered by Chest Impact–Induced Abnormalities in Repolarization. Mark S. Link. Originally published1 Apr 2012https://doi.org/10.1161/CIRCEP.111.962712Circulation: Arrhythmia and Electrophysiology. 2012;5:425–432
Commotio Cordis pathophysiology :
- Commotio Cordis is a diagnosis of exclusion.
- Commotio Cordis is a primary arrhythmic event that occurs when the mechanical energy generated by a stroke is limited to a small area of the precordium (usually over the left ventricle) and profoundly alters the electrical stability of the myocardium, resulting in ventricular fibrillation.
- In the majority of cases (58%), the patient is struck in the chest by a projectile, commonly thrown, thrown, or struck, and the velocity of the projectile is estimated to be 30 to 50 mph at the time of impact.
- The impact occurs within a specific 10 to 30 millisecond portion of the cardiac cycle. This period occurs in the ascending phase of the T wave, when the ventricular myocardium is repolarizing, during the transition from systole to diastole (relaxation). This small window of vulnerability makes commotio cordis a very rare event.
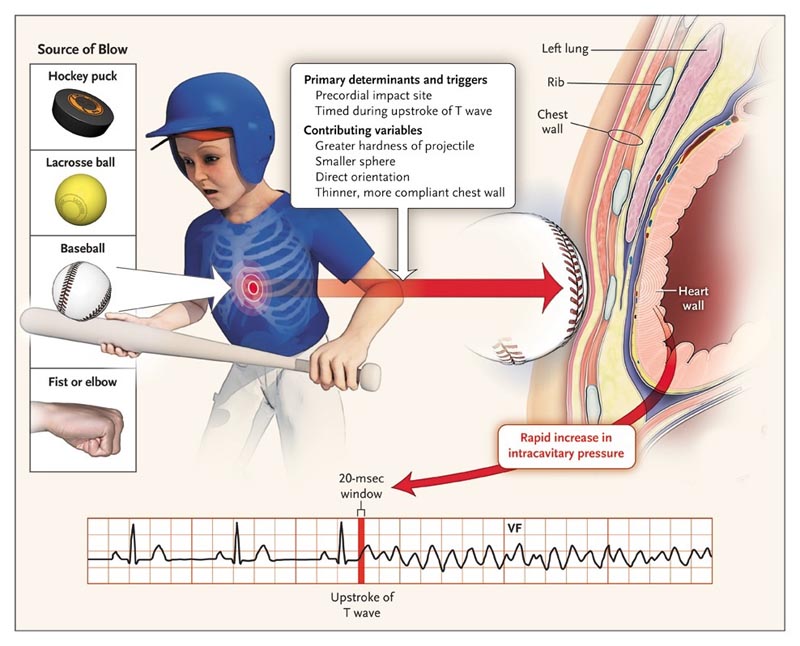
Figure : Pathophysiology of Commotio Cordis. In recreational and competitive sports, chest hits may involve balls or pucks or may be inflicted through body contact. The location of the blow to the chest and its timing in relation to the cardiac cycle are the main determinants of commotio cordis. Other factors that may contribute to the risk of an event include the density, size and orientation of the projectile and the shape of the chest; Younger people are the most vulnerable due to their thinner and less developed ribcage and musculature.
Clinical presentation of commotio cordis:
|
Prevention of Commotio Cordis :
Chest protectors have been studied extensively and are recommended for use during sports such as baseball and softball. Unfortunately, there is no evidence to support thoracic shields as an effective means of reducing the impact of blow to the vulnerable precordium or decreasing the incidence of commotio cordis . For a chest protector to be effective, it must be amply padded and supported, which greatly hinders athletic performance by limiting the player’s movement. 18% of people who suffered commotio cordis wore a chest shield.
Having public access to defibrillators at sporting events with a high incidence of commotio cordis and training people in the use of defibrillators and cardiopulmonary resuscitation can help improve survival rates for people who suffer sudden cardiac arrest.
Public education on the importance of preventing precordial strokes. For example; Baseball and softball coaches are encouraged to educate players to step away or turn using the right shoulder to deflect balls rather than the chest wall.
Summary The general public and medical community have become more aware of commotio cordis as a major cause of sudden death. Commotio cordis occurs in healthy, active young people, typically during recreational and competitive sports, but in some cases even during normal daily activities. A variety of experimental models indicate that if administered at a particular time in the cardiac cycle, even seemingly innocent precordial blows can trigger ventricular fibrillation and lead to fatal commotio cordis events . More efforts are needed to prevent these largely avoidable deaths by providing more education, better-designed sports equipment (e.g., effective chest wall protectors), and broader access to AEDs at organized sporting events. These strategies should result in a safer sporting environment for our youth. |
Report from the American Heart Association (AHA) on the Damar Hamlin case

Understanding cardiac arrest and the emergency response following Damar Hamlin’s collapse during Monday Night Football
While playing in the Buffalo Bills - Cincinnati Bengals game on Monday Night Football on January 2, Bills player Damar Hamlin went into cardiac arrest after a hit and was administered CPR on the field before being taken to a hospital. area hospital. according to an overnight statement from the Buffalo Bills.
Explanation of on-site care
Hamlin reportedly experienced cardiac arrest, when the heart stops abruptly with little or no warning. Early recognition of cardiac arrest improves the person’s chances of survival and is key to initiating proper CPR care and appropriate use of defibrillation to restart the heart. The medical team on scene assessed the situation and appeared to quickly remove the safety pads, begin CPR, and apply the automated external defibrillator (AED).
CPR can help keep the heart pumping and blood flowing to vital organs until a shock from a defibrillator is available to restore normal heart rhythm. The patient can then be safely transported to receive additional medical treatment, supportive care, testing to determine what may have been the cause of the arrest, and recovery, including physical and mental health resources for the individual and their family.
Possible causes
Cardiac arrest can have several causes. Since Hamlin collapsed immediately after a tackle on the play, a possible cause could be commotio cordis. Commotio cordis is a rare phenomenon of a sudden blunt force impact to the chest causing sudden death in the absence of apparent heart damage. Hitting the chest at precisely the wrong time in the cardiac cycle causes an electrical abnormality in the heart resulting in an irregular heart rhythm that cannot pump blood to the body. Immediate CPR and a shock to restore rhythm can help the heartbeat return to normal.
Another cause of cardiac arrest that additional testing is likely to try to detect or rule out is hypertrophic cardiomyopathy (HCM), or a thickened heart muscle, a more common cause of sudden cardiac death specifically in young people and athletes. A thickened heart may be due to a genetic condition or may be caused by sports conditioning that thickens the heart muscles and may make you more susceptible to an irregular heart rhythm such as ventricular fibrillation/tachycardia.
Traumatic stress for first responders, observers
Witnessing and responding to cardiac arrest can be a very traumatic event and can cause lingering psychological impact, regardless of the outcome. Lay responders and witnesses may need support and resources to help them process their experience.
Respondents mentioned exhaustion, guilt, flashbacks, sleep disorders, self-doubt, anger, sadness, and fear. A positive outcome from performing CPR may mitigate some of the emotional responses; however, psychological responses are broad and individualized. In situations with a failed resuscitation attempt, PTSD symptom scores were twice as high for responders as for non-witnesses.
“This was traumatic for everyone, especially Hamlin’s family and teammates, but also for many others involved in and witnesses to the event. More than 70% of cardiac arrests that do not occur in the hospital occur in a home where access to medical professionals and an AED is not as readily available,” said Mariell Jessup, MD, FAHA, chief scientific and medical officer of the American Heart Association. “Recognizing cardiac arrest, calling 911 immediately, performing CPR, and using an AED as soon as it is available are critical to survival. Statistically speaking, it is likely that the person will need the help of a family member or friend to survive.”
Having community members trained in CPR and AED in public spaces can increase the chances of survival. The rate of bystander CPR in North America is estimated at only 39-44%, and only 1 in 10 people survive out-of-hospital cardiac arrest. Improving the rate of bystander CPR is critical to increasing survival from out-of-hospital cardiac arrest (OHCA).
The ability to perform CPR and use a defibrillator are the fundamental components of layperson preparation to respond to cardiac arrest. People also need to feel emotionally prepared to respond and be able to deal with the consequences of performing CPR.
Resources to learn CPR
Each year in the United States, approximately 350,000 people experience sudden cardiac arrest in the community. Anyone who witnesses a cardiac arrest in the community (i.e. not in a hospital) can perform CPR. Approximately 70% of cardiac arrests that do not occur in the hospital occur in homes and private residences, so a friend or family member is likely the person to take action. CPR, especially if performed immediately, can double or triple a cardiac arrest victim’s chances of survival.
For adults and adolescent children, Hands-Only CPR is an easy-to-learn skill that requires just two steps: calling emergency services and pressing hard and fast on the center of the chest at a rate of 100 to 120 beats per minute. .
ACC Council Statement on Sudden Cardiac Arrest During Monday Night Football
On Monday night, Damar Hamlin of the Buffalo Bills experienced sudden cardiac arrest in the first quarter of the game against the Cincinnati Bengals. At this time, many details regarding this catastrophic event remain to be determined. He is reported to be in critical condition in the intensive care unit at the University of Cincinnati Medical Center. First and foremost, our hearts go out to Damar, his family, the Buffalo Bills and all the players, coaches and staff who were on the field during this terrible event. Along with everyone else, we hope for Damar’s full recovery. When catastrophes like this occur with athletes in the competitive field, we are reminded that these events, although very rare, are always emotionally traumatic for all who witness them and it is important that appropriate support and respect for privacy be provided. to all those involved. We would like to remind everyone, including medical professionals, that the etiology surrounding this cardiac arrest remains unknown and is being investigated by medical professionals at the University of Cincinnati and affiliates of the Buffalo Bills. Reckless speculation on social media is a source of misinformation and could have other unintended negative consequences. We encourage everyone to avoid this practice and allow those in charge to proceed with the medical evaluation.
At some point in the future, as more details are revealed, we will be able to learn from this event to continue to improve emergency care for athletes who suffer cardiac arrest on the field. Emergency cardiac care on the field is a critical element of sports cardiology care, and in fact, the immediate response by the Bills training staff and other medical professionals on the field Monday night is exactly what it should be. occur after such acute cardiac events. Rapid assessment of a collapsed athlete, recognition of the event as sudden cardiac arrest, and initiation of an Emergency Action Plan (EAP), including immediate cardiopulmonary resuscitation (CPR) and use of an automated external defibrillator (AED) , are the pillars of this emergency care.
Even with intensive pre-season cardiac evaluations, we will never be able to prevent all cases of sudden cardiac arrest in athletes, but emphasis on PAD and early defibrillator use has been shown to save lives.
Sudden cardiac arrest in healthy young athletes is rare, but this case illustrates the importance of close collaboration between sports leagues, players’ associations and team medical staff to prepare for these moments. This should include an annual off-season review of EAPs and regular field trials of emergency medical scenarios, which may include training by other consultants and experts. In the NFL, there is also a "60-minute huddle" one hour before each game to discuss coordination of care between medical personnel and local emergency care providers for potential on-field emergencies. An athlete’s sudden cardiac arrest reminds us that directing resources and education on effective EAP and CPR training to those caring for competitive athletes saves lives.















