Moderately severe or severe disease develops in approximately 35% of patients with acute pancreatitis, a condition that is associated with worse outcomes. In animal models, regional hypoperfusion of the pancreas is spatially correlated with necrosis and can be corrected by fluid resuscitation. Initial observational studies indicated that hemoconcentration, which is a surrogate for systemic hypovolemia, was associated with pancreatic necrosis. However, subsequent work indicated that administering a greater volume of resuscitative fluids during the first 24 hours may not improve outcomes.
Randomized controlled trials comparing different volumes of intravenous fluid, which were limited by small size and overly specific inclusion criteria, provided conflicting results. Two trials involving patients with severe pancreatitis demonstrated that rapid fluid expansion was associated with decreased survival.
A randomized trial involving patients without baseline systemic inflammatory response syndrome (SIRS), who therefore had an initially low risk of moderate to severe disease, showed more rapid clinical improvement with vigorous hydration than with moderate hydration. A systematic review, although limited by the heterogeneity and quality of the source studies, showed a lower incidence of adverse events and lower mortality with moderate hydration than with aggressive hydration.
We initiated WATERFALL (Early weight-based aggressive versus non-aggressive goal-directed fluid resuscitation in the early phase of acute pancreatitis: an open-label, multicenter, randomized controlled trial) to investigate the safety and effectiveness of aggressive fluid resuscitation. fluid resuscitation compared with moderate fluid resuscitation in a diverse sample of acute pancreatitis patients with a range of disease severity.
Background
Early aggressive hydration is widely recommended for the treatment of acute pancreatitis, but evidence for this practice is limited.
Methods
At 18 centers, we randomly assigned patients presenting with acute pancreatitis to receive aggressive or moderate goal-directed resuscitation with lactated Ringer’s solution.
- Aggressive fluid resuscitation consisted of a bolus of 20 ml per kilogram of body weight, followed by 3 ml per kilogram per hour .
- Moderate fluid resuscitation consisted of a bolus of 10 ml per kilogram in patients with hypovolemia or no bolus in patients with normovolemia, followed by 1.5 ml per kilogram per hour in all patients in this group .
Patients were evaluated at 12, 24, 48, and 72 hours, and fluid replacement was adjusted according to the patient’s clinical status. The primary outcome was the development of moderately severe or severe pancreatitis during hospitalization. The main safety outcome was fluid overload. The planned sample size was 744,
Results
A total of 249 patients were included in the interim analysis.
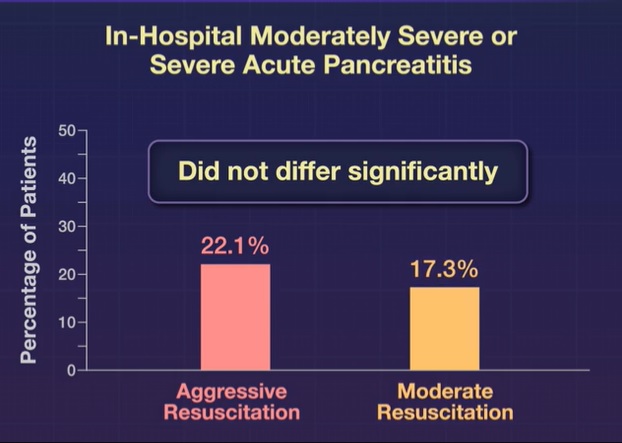
The trial was stopped due to between-group differences in safety outcomes with no significant difference in the incidence of moderately severe or severe pancreatitis (22.1% in the aggressive resuscitation group and 17.3% in the aggressive resuscitation group). moderate; adjusted relative risk, 1.30; 95% confidence interval [CI], 0.78 to 2.18; P = 0.32).
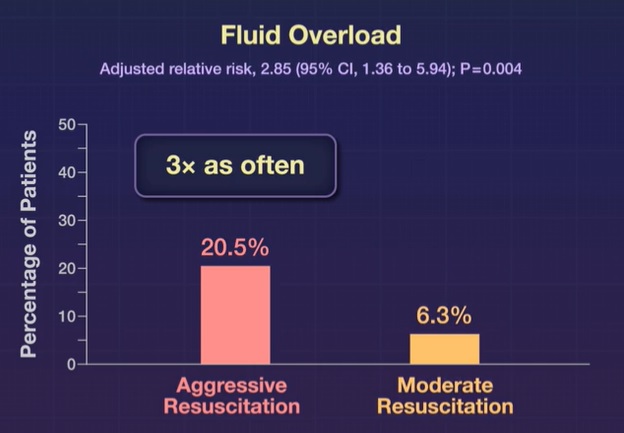
Fluid overload developed in 20.5% of patients who received aggressive resuscitation and 6.3% of those who received moderate resuscitation (adjusted relative risk, 2.85; 95% CI, 1.36 to 5.94, P = 0.004).
The median duration of hospitalization was 6 days (interquartile range, 4 to 8) in the aggressive resuscitation group and 5 days (interquartile range, 3 to 7) in the moderate resuscitation group.
Conclusions In this randomized trial involving patients with acute pancreatitis, early aggressive fluid resuscitation resulted in an increased incidence of fluid overload without improvement in clinical outcomes. |
Discussion
This trial showed that aggressive fluid resuscitation increased the risk of volume overload. Given data showing increased harm without improvement with respect to the primary outcome, the data and safety monitoring board unanimously recommended that the trial be stopped. These findings do not support current management guidelines, which recommend early aggressive resuscitation for the treatment of acute pancreatitis.
An increased risk of fluid overload was detected in the overall patient population and also in subgroups of patients without SIRS at baseline, patients with SIRS at baseline (thus at increased risk of developing severe pancreatitis), and patients with hypovolemia. Although most episodes of fluid overload with aggressive hydration were not severe (the trial was designed to allow early detection and treatment), this was not balanced by an improvement in outcomes. In this interim analysis, no significant differences were found between groups in the risk of moderately severe or severe acute pancreatitis (primary outcome). Intensive fluid resuscitation was associated with a trend toward greater symptom intensity and longer duration of treatment. hospital stay and a higher incidence of necrotizing pancreatitis than moderate fluid resuscitation.
The absence of an efficacy signal for aggressive hydration is of practical importance as it challenges a strong predilection in many clinicians for the use of early high-volume hydration.
The WATERFALL findings add to the growing body of evidence that aggressive hydration is linked to worse outcomes in critically ill patients. Pancreatitis is associated with increased intra-abdominal pressure, which may be worsened by excess intravenous fluids; This adverse effect of aggressive fluid resuscitation may explain the trend toward greater symptom intensity. The largest difference in the volume of fluid administered occurred in the first 12 hours, corresponding to the difference in symptoms at this time.
In summary: In our randomized evaluation of aggressive fluid resuscitation compared with moderate fluid resuscitation for the treatment of acute pancreatitis, the use of aggressive fluid resuscitation led to an increased risk of volume overload and did not show the hypothetical benefit on disease-specific outcomes.
(Funded by the Carlos III Health Institute and others; WATERFALL ClinicalTrials.gov number, NCT04381169. opens in a new tab.)















