According to study results published in JAMA Neurology , atrial fibrillation detection with implantable loop recorder did not significantly reduce the risk of stroke compared with usual care.
“Stroke is a leading cause of mortality and disability worldwide,” wrote Soren Zoga Diederichsen, MD, PhD, of the department of cardiology at Copenhagen University Hospital in Denmark, and colleagues. “Atrial fibrillation is an important and often undiagnosed risk factor for stroke.”
Severity and etiology of incident stroke in patients screened for atrial fibrillation versus usual care and the impact of prior stroke . Key points Can atrial fibrillation screening with implantable loop recorder reduce the risk of serious stroke in people with risk factors or a previous stroke? Findings In this post hoc analysis of a randomized clinical trial that included 6004 participants at high risk for stroke and 1056 with a prior stroke, loop recorder screening did not result in a significant reduction in disabling or fatal strokes compared with usual care in all participants or among participants with a previous stroke. The vast majority of strokes were ischemic, but cardioembolism was relatively rare. Meaning that screening for atrial fibrillation with implantable loop recorder in high-risk people did not result in a significant reduction in the risk of serious stroke. |
Importance
Atrial fibrillation (AF) screening trials have failed to demonstrate a significant reduction in stroke risk. The impact on stroke severity and the significance of previous strokes is unknown.
Aim
To evaluate stroke characteristics in patients undergoing AF screening with an implantable loop recorder (ILR) versus usual care and evaluate the significance of prior stroke.
Design, environment and participants
This was a post hoc analysis of the randomized clinical trial Atrial Fibrillation Detected by Continuous Electrocardiogram with Implantable Loop Recorder to Prevent Stroke in High-Risk Individuals (LOOP). People aged 70 years or older without known AF but diagnosed with one or more of the following, hypertension, diabetes, heart failure, or previous stroke, were selected for inclusion. Four sites in Denmark recruited participants by letter between January 31, 2014 and May 17, 2016. The median (IQR) follow-up period was 65 (59-70) months. Data was analyzed from April 1 to May 31, 2022.
Interventions
Detection of ILR for AF and initiation of anticoagulation if AF duration of 6 minutes or longer was detected (ILR group) versus usual care (control group).
Main results and measures
Adjudicated stroke, classified according to the modified Rankin Scale (mRS) using a score of 3 or greater as the cut-off point for severe stroke (disabling or fatal), and according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification for ischemic strokes.
Results
A total of 6205 people were selected for inclusion, and 6004 were randomized and included in the analysis; 4503 participants (75%; mean [SD] age, 74.7 [4.1] years; 2375 men [52.7%]) were assigned to the control group and 1501 participants (25%; mean [SD] age, 74.7 [4.1] years; 792 men [52.8%]) were assigned to the ILR group. A total of 794 of 4503 participants (17.6%) in the control group had a history of prior stroke compared with 262 of 1501 participants (17.5%) in the ILR group.
During follow-up, 1027 participants were diagnosed with AF (control group, 550 [12%] vs ILR group, 477 [32%]), and anticoagulation was started in 89% of these (910). A total of 315 participants (5.2%) had a stroke (control group, 249 [5.5%] vs. ILR group, 66 [4.4%]), and the mean (IQR) mRS score was 2 (1-3) with no difference across groups. P = 0.07) and 0.69 (95% CI, 0.44-1.09; P = 0.11), respectively. For participants without prior stroke, the hazard ratios were 0.68 (95% CI, 0.48 to 0.97; P = 0.04) and 0.54 (95% CI, 0.30). to 0.97; P = 0.04), respectively.
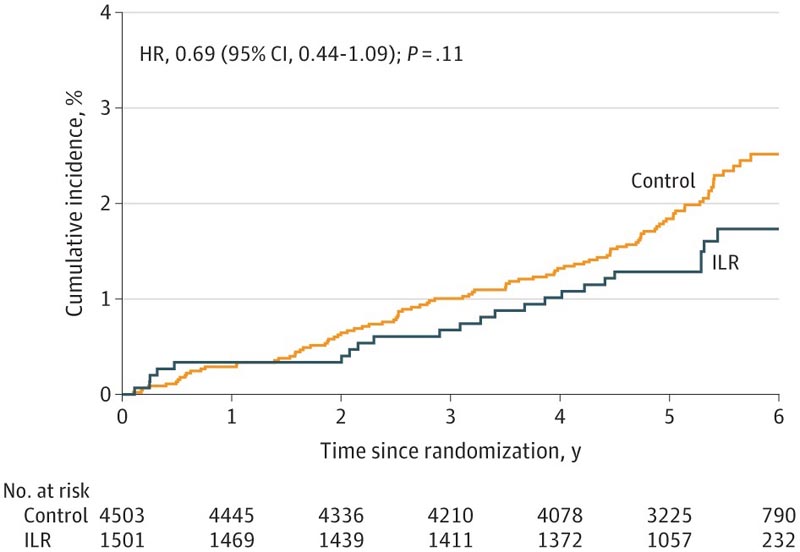
Figure : Cumulative incidence of severe stroke. Cumulative incidence curves for disabling or fatal stroke (modified Rankin Scale [mRS] score ≥3) are compared in the control group and the implantable loop recorder (ILR). HR indicates the risk ratio.
Conclusions and relevance
This post hoc analysis of the LOOP randomized clinical trial found that AF screening with ILR did not result in a significant decrease in ischemic or severe stroke compared with usual care. Exploratory subgroup analyzes indicated a possible reduction in these outcomes among participants without prior stroke.















