
Key points What are the clinical outcomes of different factors associated with the imbalance between oxygen supply and demand among patients with type 2 myocardial infarction? Findings In this secondary analysis of a randomized clinical trial, tachyarrhythmia was the most common factor associated with imbalance between oxygen supply and demand, occurring in 55% of all patients with type 2 myocardial infarction , and was associated with best results. Systemic diseases associated with type 2 myocardial infarction , presenting with anemia, hypoxemia, hypotension, or severe hypertension, were less common, but patients with these diseases shared similar characteristics and had the highest rates of death from all causes. Meaning Underlying factors associated with the imbalance between oxygen supply and demand among patients with type 2 myocardial infarction may provide useful prognostic information. |
The definition of myocardial infarction has evolved due to the improved sensitivity of cardiac biomarkers. The Fourth Universal Definition of Myocardial Infarction classifies type 1 myocardial infarction as due to thrombotic occlusion following rupture or erosion of atherosclerotic plaque and type 2 myocardial infarction as due to imbalance between supply and demand of myocardial oxygen in the setting of acute systemic or cardiac disease or an underlying coronary mechanism other than plaque rupture.
It is recognized that type 2 myocardial infarction is common and is associated with a substantial risk of adverse clinical outcomes, with only 30% of patients alive at 5 years. Despite this fact, strategies for the investigation and management of type 2 myocardial infarction have not been defined.
Type 2 myocardial infarction is a heterogeneous condition that encompasses multiple factors associated with reduced myocardial oxygen delivery (coronary embolism, dissection or vasospasm, hypotension, hypoxemia, and anemia) and increased myocardial oxygen demand (hypertension and tachyarrhythmia). ). These etiological factors may confer different risks of adverse clinical outcomes and require different treatment strategies.
In this secondary analysis of a multicenter randomized clinical trial we report the frequency of these factors associated with the imbalance between oxygen supply and demand among patients with type 2 myocardial infarction, and compare their characteristics and outcomes with those of patients with type 1 myocardial infarction.
Summary
Importance
Type 2 myocardial infarction occurs due to multiple factors associated with the imbalance between myocardial oxygen supply and demand, which may confer different risks of adverse outcomes.
Aim
To evaluate the prevalence and outcomes of different factors associated with the imbalance between oxygen supply and demand in patients with type 2 myocardial infarction.
Design, environment and participants
In this secondary analysis of a stepped cluster randomized clinical trial conducted in 10 secondary and tertiary care hospitals in Scotland, 6096 patients with an adjudicated diagnosis of type 1 or type 2 myocardial infarction from June 10, 2013, to June 3 March 2016, and the findings were reported on August 28, 2018.
The trial enrolled consecutive patients with suspected acute coronary syndrome. The diagnosis of myocardial infarction was adjudicated according to the Fourth Universal Definition of Myocardial Infarction and the primary factor associated with the imbalance between oxygen supply and demand in type 2 myocardial infarction was defined. This secondary analysis was not prespecified. The statistical analysis was carried out from July 7 to 30, 2020.
Intervention
Implementation of a high-sensitivity cardiac troponin I assay.
Main results and measures
Death from all causes at one year according to factors associated with the imbalance between oxygen supply and demand in patients with type 2 myocardial infarction.
Results
Of 6,096 patients (2602 women [43%]; median age, 70 years [IQR, 58-80 years]), 4981 patients had type 1 myocardial infarction and 1115 patients had type 2 myocardial infarction.
The most common factor associated with imbalance between oxygen supply and demand was tachyarrhythmia (616 of 1115 [55%]), followed by hypoxemia (219 of 1115 [20%]), anemia (95 of 1115 [9%] ]), hypotension (89 of 1115 [8%]), severe hypertension (61 of 1115 [5%]), and coronary mechanisms (35 of 1115 [3%]).
At 1 year , all-cause mortality occurred in 15% of patients (720 of 4981) with type 1 myocardial infarction and in 23% of patients (285 of 1115) with type 2 myocardial infarction .
Compared with patients with type 1 myocardial infarction , those with type 2 myocardial infarction due to hypoxemia (adjusted odds ratio [aOR], 2.35; 95% CI, 1.72-3.18) and anemia (aOR , 1.83; 95% CI, 1.14-2.88) had the highest risk of death , while those with type 2 myocardial infarction due to tachyarrhythmia (aOR, 0.83; 95% CI, 0 .65-1.06) or coronary mechanisms (aOR, 1.07; 95% CI, 0.17-3.86) had a similar risk of death to patients with type 1 myocardial infarction.
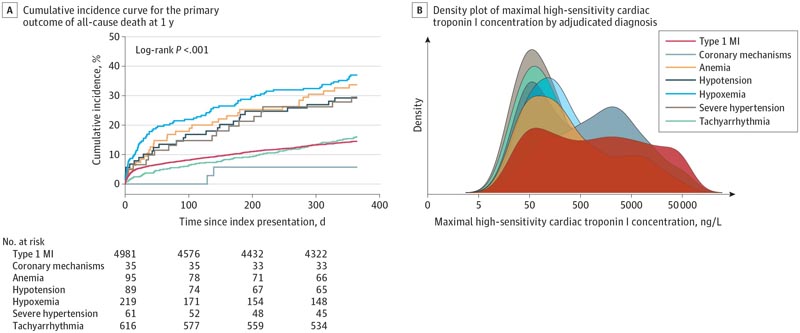
A, Cumulative incidence curve for the primary outcome of death from all causes at 1 year. B, Kernel density plot showing the distribution of peak high-sensitivity cardiac troponin I concentrations (ng/L [to convert to micrograms per liter, multiply by 0.001]) according to the adjudicated diagnosis and factors associated with the imbalance between Oxygen supply and demand in type 2 myocardial infarction (MI).
Type 2 MI related to hypoxemia or anemia carries a higher risk of 1-year mortality than type 1 MI.
Conclusions and relevance
In this secondary analysis of a randomized clinical trial, mortality after type 2 myocardial infarction was associated with the underlying etiological factor associated with the imbalance between oxygen supply and demand.
The majority of type 2 myocardial infarctions were associated with tachyarrhythmia , with a better prognosis, while hypoxemia and anemia represented a third of the cases, with double the mortality than type 1 myocardial infarction.
Clinicians should take these differential outcomes into account when determining which cases should be treated to improve patient outcomes.
Comments
Type 2 myocardial infarction ( MI) is due to an imbalance between myocardial oxygen supply and demand, which is caused by several underlying factors. It is not clear whether these different etiologies carry different prognoses.
In a secondary analysis of clinical trial data, researchers examined the prevalence and outcomes of different factors associated with imbalance between oxygen supply and demand in patients with type 2 myocardial infarction.
Among 6096 patients (median age, 70 years; 43% women) with an adjudicated type 1 or type 2 myocardial infarction, 1115 patients had a type 2 myocardial infarction. Compared with patients with type 1 myocardial infarction, those with type 2 myocardial infarction were older and had more comorbidities, including higher rates of cardiovascular disease and kidney disease.
In patients with type 2 MI, the most common factor associated with imbalance between oxygen supply and demand was tachyarrhythmia (55%), followed by hypoxemia (20%), anemia (9%), hypotension (8%). , severe hypertension (5%). ), and coronary mechanisms such as spasm or dissection (3%). At 1 year, the all-cause mortality rate was 23% in patients with type 2 MI and 15% in those with type 1 MI.
In univariate analysis, hypoxemia, anemia, severe hypertension, and hypotension were each associated with increased odds of death at 1 year. In multivariate analysis, compared with patients with type 1 MI, those with type 2 MI had higher odds of mortality from underlying factors of hypoxemia (adjusted odds ratio, 2.35) and anemia (aOR, 1.83), but not from tachyarrhythmia or coronary mechanisms (aOR of 0.83 and 1.07, respectively).
These data confirm the poor prognosis associated with type 2 myocardial infarction and reveal the variation in outcome related to the underlying etiology of the imbalance between oxygen supply and demand.
Deaths among patients with type 2 myocardial infarction are equally likely to have cardiovascular or noncardiovascular causes and often reflect the patient’s underlying systemic disease. These findings suggest that management should primarily address the underlying systemic disease and factors associated with the imbalance between oxygen supply and demand.
ClinicalTrials.gov Trial Registration Identifier: NCT01852123















