Background
The practice of sports cardiology commonly involves the evaluation of athletes for genetically determined cardiac diseases that may predispose to malignant arrhythmias, heart failure, and sudden cardiac death (SCD). High-level exercise can lead to electrical and structural cardiac remodeling that mimics inherited cardiac conditions (CHF), often referred to as the "gray zone . " Differentiating between ’athlete’s heart’ and pathology can be challenging and often requires the full arsenal of available research.
Genetic studies over the past 30 years have identified many of the genetic variants underlying CHF, and technological advances have transformed genetic testing into a more readily available and affordable clinical tool that can aid in diagnosis, treatment, and prognosis. The role of genetic testing in the evaluation and management of athletes with suspected cardiac conditions is often unclear beyond the context of specialized cardiogenetics centers.
Summary
The practice of sports cardiology commonly involves the evaluation of athletes for genetically determined heart diseases that may predispose to malignant arrhythmias, heart failure, and sudden cardiac death. High-level exercise can lead to electrical and structural cardiac remodeling that mimics inherited cardiac conditions (CHF).
Differentiating between “athlete’s heart” and pathology can be challenging and often requires the full arsenal of available research. Genetic studies over the past 30 years have identified many of the genetic variants underlying CHF, and technological advances have transformed genetic testing into an affordable and more readily available clinical tool that can aid in diagnosis, treatment, and prognosis. The role of genetic testing in the evaluation and management of athletes with suspected cardiac conditions is often unclear beyond the context of specialized cardiogenetics centers.
This document is intended for physicians, nurses, and allied health professionals involved in athlete care. Given the increasing role and availability of genetic testing, this document was created to address the needs of the broader sports cardiology community, the majority of whom work outside of specialized cardiogenetics centers, when faced with to the evaluation and management of athletes with suspected CCI.
The first part of the document provides an overview of the terminology and basic principles and offers guidance on the appropriate use of genetic testing in the evaluation of such athletes. It outlines key considerations when considering genetic testing, highlighting potential benefits and dangers, and provides a roadmap for genetic testing.
The second part of the document presents common clinical scenarios in the practice of sports cardiology, highlighting the diagnostic, prognostic and therapeutic implications of genetic testing, including the impact on exercise recommendations. The scope of this paper does not extend to a complete description of the genetic basis, research, or management of CHF.
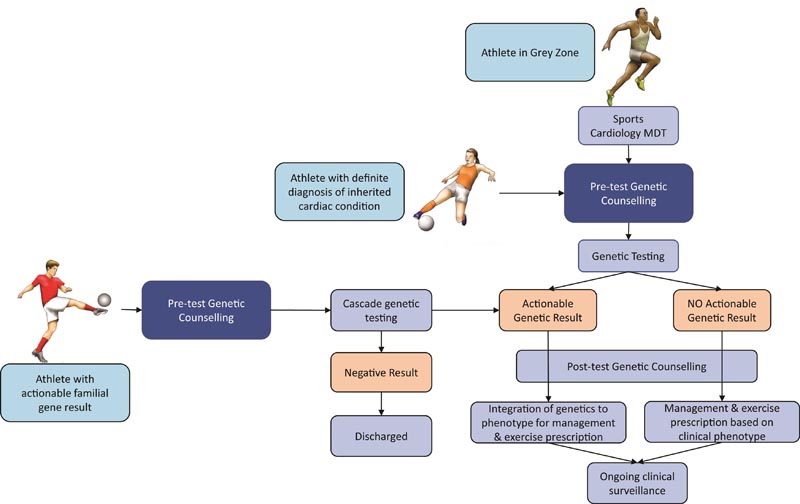
Graphical Summary : Flowchart showing pathways for athletes to proceed with cardiac genetic testing depending on whether they have a known hereditary heart condition (CHF) diagnosis, are a gray zone athlete, or have a known actionable genetic result ( pathogenic or probably pathogenic) in your family The multidisciplinary should consist of people with experience in sports cardiology, cardiac genetics, and the diagnosis and management of CHF and genetic counselors.
Comments
Recommendations on how to use genetic testing to prevent sudden cardiac death in athletes and enable safe exercise are published in the European Journal of Preventive Cardiology , a journal of the European Society of Cardiology (ESC).
"Genetic testing for potentially lethal variants is more accessible than ever and this paper focuses on which athletes should be tested and when," said author Dr. Michael Papadakis of St George’s, University of London, UK.
“Athletes should be counseled about possible results before genetic testing, as it could mean exclusion or restriction from playing.”
In most cases, clinical assessment will dictate the need for preventive therapy such as a defibrillator and advice on exercise and participation in competitive sports. Dr. Papadakis explained: “Even if a genetic abnormality is found, recommendations regarding treatment and return to play generally depend on the clinical severity of the disease. Is it causing symptoms like fainting? Is the heart excessively weak or large? We can see many heart rhythm irregularities (arrhythmias) and do they get worse during exercise? If the answer is ’yes’ to any of these questions, the game will likely be restricted in some way."
One example is an inherited condition that can cause sudden cardiac death in athletes called hypertrophic cardiomyopathy (HCM), in which the heart muscle is abnormally thick. Dr Papadakis noted: “We used to be very conservative, but now our advice is more liberal. Athletes with HCM should undergo a comprehensive clinical evaluation to assess their risk of sudden cardiac death and then receive an exercise prescription. Genetic testing in this condition does not affect management in most cases. Asymptomatic athletes considered low risk can potentially participate in competitive sports after an informed discussion with their doctor. Others at higher risk may be restricted to moderate intensity exercise. The exercise prescription should be as specific as possible and describe how often, for how long, at what intensity, and what exercise or sport is safe.”
In some cases, however, genetic testing can dictate management. An example is long QT syndrome (LQTS), which is an inherited electrical fault of the heart. Identification of different genetic subtypes (LQT 1-3) can inform the risk of arrhythmias, identify potential triggers that should be avoided, and help guide medical therapies and exercise planning. Dr Papadakis said: "For example, sudden immersion in cold water is more likely to cause life-threatening arrhythmias in LQT type 1 rather than types 2 or 3, so more care should be taken in swimmers who have the type 1 genetic subtype that runners.”
The only situation in which genetic testing alone can result in exclusion from the game is a condition of the heart muscle called arrhythmogenic cardiomyopathy (ARVC). “Even if an athlete has no clinical evidence of the disease but has the gene for the condition, he should refrain from playing competitive and high-intensity sports ,” Dr. Papadakis said. “This is because studies show that people with the gene who exercise at a high level tend to develop the disease earlier in life and tend to develop a more severe disease that can cause a life-threatening arrhythmia during sport.” ”.
Pre-test genetic counseling should be performed to discuss the implications for athletes and their families. As an example, an athlete’s mother is clinically diagnosed with ARVC and has the causative gene, then the athlete is examined and all clinical tests are normal. The athlete has two options: 1) clinical follow-up, probably annually, to detect signs of disease; or 2) genetic testing. “The athlete needs to know that if the test is positive, that may indicate the end of his career , even if there is no clinical evidence of illness,” Dr. Papadakis said. “On the other hand, if genetic testing is refused, the condition may worsen. “Post-test counseling is critical given the potential psychosocial, financial and mental health implications, especially if the athlete is excluded from the game.”
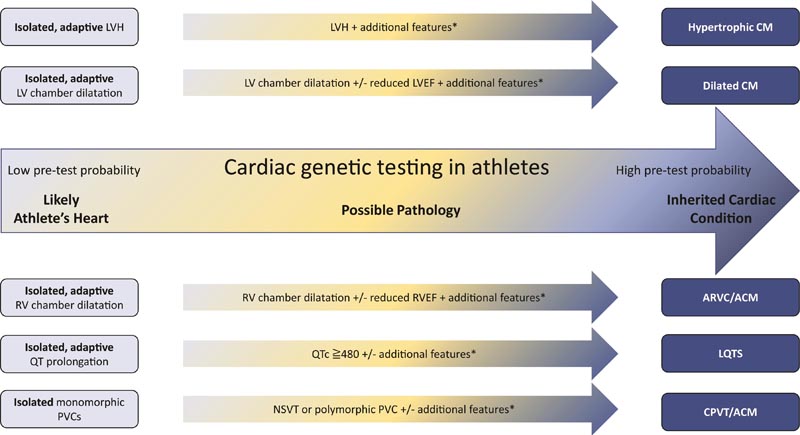
Schematic representation of the utility of genetic testing in sports cardiology for some of the common clinical scenarios, including the "gray zone." The system is based on the pre-test probability of positive performance across the spectrum with adaptive changes on the left due to exercise where genetic testing should not be used and on the right an established diagnosis of an inherited heart condition when it should be performed. genetic testing. done. A multidisciplinary team discussion is paramount when genetic testing is considered in the “gray zone” represented by the arrows.
For child athletes, genetic counseling at an expert pediatric center with the assistance of a child mental health specialist may be necessary. Dr Papadakis noted: “The psychological impact of a positive genetic test result can be significant for the child, especially if this leads to sports exclusion, even in the absence of clinical disease as in ARVC.”
In children with a clinical diagnosis of an inherited condition, genetic testing can confirm the diagnosis and, in some cases, help predict the risk of sudden death during sports. For example, having the gene for a heart electrical fault called catecholaminergic polymorphic ventricular tachycardia (CPVT) can lead to recommending preventive therapies, such as beta blockers, and dictate decisions about exercise. “This is important as CPVT predisposes to arrhythmias during exercise and can lead to sudden death at a very young age,” Dr. Papadakis said. “In contrast, the timing of genetic testing in children with a family history of HCM is controversial since, in the absence of clinical signs, it rarely causes sudden death in infancy.”
The scientific statement was prepared by the Exercise and Sports Cardiology Section of the European Association for Preventive Cardiology, the European Heart Rhythm Association, the ESC working group on myocardial and pericardial diseases, the Cardiovascular Genomics Council of the ESC, the European Society of Human Genetics and the European Association of Pediatric and Congenital Cardiology.















