Patients with sacroiliac joint (SIJ) pain primarily present with joint pain in the lower back and/or the back of the hips. Accurately diagnosing SIJ pain is an ongoing problem faced by pain management physicians, as the exact source of the pain is often difficult to determine.
Bernard et al. It has been estimated that 70-80% of the population complains at least once of low back pain, of which 15-30%, the main pain generator is the SIJ.
Additionally, many symptoms and clinical signs of SIJ-related pain are present in other causes of low back pain.
SIJ pain can be due to both intra-articular and extra-articular causes .
Examples of intra-articular causes include infection, arthritis, spondyloarthropathies, trauma, malignancy, and cystic disease, while extra-articular causes include enthesopathy, fractures, ligament injuries, myofascial disorders, and pregnancy. However, in clinical practice the most common cause of SIJ pain remains idiopathic .
SIJ-mediated pain usually manifests as pain in the gluteal region in 94% of patients. Pain may also refer to the lower lumbar region (72%), groin (14%), upper lumbar region (6%), and abdomen (2%).
To date, there have been no acceptable and accurate diagnostic criteria or standard of care for the treatment of sacroiliac joint (SIJ) pain. Several studies have yielded different contributions of clinical presentation, history, and physical examination in the diagnosis of SIJ pain.
Our objective in this study is to evaluate the sensitivity and specificity of clinical diagnostic tests and their predictive value for accurately diagnosing SIJ pain.
Methodology
Upon enrolling 200 eligible patients with SIJ pain as their primary diagnosis, they were reevaluated and their verbal rating scale (VRS) pain score and demographic data were obtained.
Subsequently, three SIJ diagnostic tests were performed: “thigh push test,” “Patrick test,” and a modified version of the Gaenslen test that is known as the “Mekhail test.”
Patients were then taken to the procedure room for SIJ injection, the confirmatory result of which was ≥50% pain relief.
The doctors who performed the procedure did not know the results of the 3 tests performed.
The results of the 3 tests were incorporated with the results of the procedure from which we extracted statistical and medical conclusions that determined their predictive value and the degree of help to physicians in the diagnosis of SIJ pain.
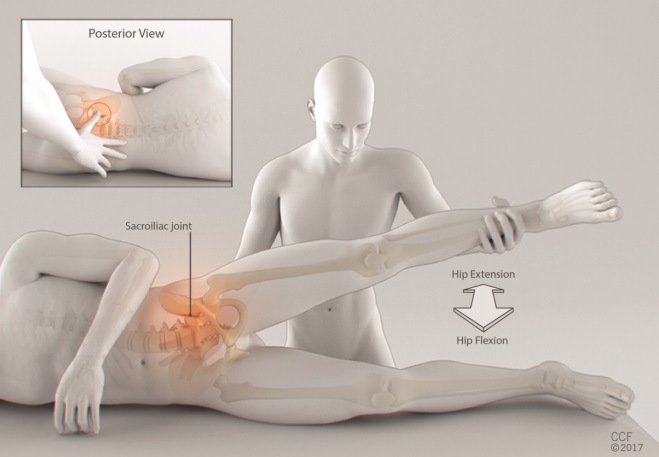
Thigh thrust test : The patient is placed supine on the examination table with the hip flexed 90º. The examiner stands at the bedside on the patient’s painful side and provides a quick push on the line of the femur to create a shear stress on the SIJ while the other arm stabilizes the sacrum. Patrick’s test: The patient is placed supine on the examination table while the patient flexes, abducts, and externally rotates the hip on the affected side. The examiner stabilizes the pelvis by placing a hand on the opposite anterior superior iliac spine (ASIS) while a downward force applied to the painful extremity creates a pulling force on the anterior SIJ. Mekhail test (Figure 1): The Mekhail test works similarly to the Gaenslen test in that it places stress on the SIJ, however, it has the advantage of avoiding the muscle protective effect that patients exert in association with the Gaenslen test. The patient should lie on the non-painful side rather than on his or her back on the edge of the bed. The examiner then stabilizes the pelvis and passively flexes and overextends the hip of the painful lower extremity (with the knee extended) while palpating the SIJ, creating a shear stress on the SIJ. The test was considered positive if the pain was reproduced only with extreme extension movement and relieved by forward flexion movement.
|
Patients were subsequently transferred to the procedure room where the SI joint injection was performed by a physician who was blinded to the results of the previous SIJ provocation tests. The X-ray-guided SIJ injection procedure was consistently performed identically each time to standardize the results.
Results
We found that the cumulative effect of adding simultaneous testing increased test sensitivity but decreased specificity , creating a powerful screening tool.
The combination of Partick and Mekhail tests demonstrated the best accuracy with 94% sensitivity, 17% specificity, 81% PPV, and 44% NPV.
The Patrick test was better than other tests in discriminating SIJ from non-SIJ patients.
No combination produced both significant sensitivity and specificity.
Overall, the overall predictive value of any of the tests alone or their combination did not vary significantly from the predictive value of baseline demographic data, including preinjection pain score and pain baseline diagram.
Conclusion
In conclusion, the results of our study were similar to the publications of several authors, who found that physical examination plays a limited role in the diagnosis of SIJ pain.
Specifically, we found that clinical tests and/or their combinations did not add significant predictive power compared to patients’ baseline characteristics in predicting response to diagnostic sacroiliac joint injection, although combinations of the Mekhail and Patrick tests They yielded a high sensitivity (94%), making them viable for screening, possibly consecutively reducing unnecessary diagnostic costs of SIJ injection procedures.















