
Huang and colleagues recently reported that up to 76% of patients discharged after hospitalization for COVID-19 had at least one symptom persisting 6 months after illness onset, including fatigue or muscle weakness (63% ), sleeping difficulties (26%), and anxiety or depression (23%). Furthermore, more than 50% of patients had abnormal chest CT images indicating impaired lung function.
Although SARS-CoV-2 primarily affects the lungs, many other organs are also affected. Enteric symptoms are common in COVID-19, and gastrointestinal symptoms may be the only symptom, or may be present before respiratory symptoms. The SARS-CoV-2 cellular receptor, ACE2, is highly expressed in the intestine and SARS-CoV-2 has been observed in the colon tissue and stool of COVID-19 patients.
Therefore, we examined the long-term gastrointestinal sequelae of SARS-CoV-2 infection in patients admitted with COVID-19 to 12 hospitals in Hubei and Guangdong provinces, China, between January 16 and January 7. March 2020, and were subsequently discharged.
117 discharged COVID-19 patients (53 [45%] of whom were 60 years or older) completed a return visit (usually 1 month after discharge) and a telephone interview around 90 days after discharge. high.
The most frequent symptoms upon admission were:
- Fever (79 [69%] of 114 patients)
- Cough (77 [66%] of 117 patients)
- Dyspnea 20 (17%) of 117 patients.
Gastrointestinal symptoms were recorded in 15 (13%) of 117 patients on admission and in 49 (42%) of 117 patients during hospitalization.
The median length of hospital stay was 19 days (IQR 16-23), during which the majority of patients (102 [87%] of 117) required supplemental oxygen; 24 (22%) of 111 patients had decreased blood oxygen saturation; 33 (28%) of 117 were seriously ill; and 28 (24%) of 117 required admission to the intensive care unit.
Gastrointestinal sequelae were defined as gastrointestinal symptoms that occurred after discharge, but were not present during the month before COVID-19 onset. 52 (44%) of 117 patients reported gastrointestinal symptoms after discharge at the 90-day telephone interview, of whom 51 patients had gastrointestinal symptoms at 90 days after discharge and one had gastrointestinal sequelae that had resolved at follow-up. 90 days.
The most frequent gastrointestinal sequelae in 117 patients were:
- Loss of appetite (28 [24%] patients).
- Nausea (21 [18%]).
- Acid reflux (21 [18%]).
- Diarrhea (17 [15%]).
Less common gastrointestinal sequelae included abdominal distension (16 [14%] patients), belching (12 [10%] patients), vomiting (11 [9%]), abdominal pain (eight [7%]), and bloody stools ( two 2%]).
None of the 65 patients without gastrointestinal sequelae at 90 days presented gastrointestinal symptoms on admission or during hospitalization.
Of the 52 patients with gastrointestinal sequelae after discharge, 15 (29%) had gastrointestinal symptoms on admission and during hospitalization, 34 (65%) had such symptoms during hospitalization, and three (6%) had such symptoms only after discharge. .
Patients with gastrointestinal sequelae at 90 days were similar in age, sex, body mass index, and incidence of comorbidities to those without gastrointestinal sequelae, and had a similar length of hospital stay.
The results of blood tests on admission showed that the leukocyte count, neutrophil count, and procalcitonin concentration were higher in patients with gastrointestinal sequelae at 90 days, although the values in both groups were in the normal range. .
C-reactive protein concentrations were higher in patients with gastrointestinal sequelae at 90 days than in those without gastrointestinal sequelae.
90 days after discharge, blood tests showed that alanine aminotransferase was higher in patients with gastrointestinal sequelae.
No other differences were observed; procalcitonin and C-reactive protein were not tested at 90 days.
Compared with patients without gastrointestinal sequelae at 90 days, patients with gastrointestinal sequelae more frequently presented dyspnea (23% vs 12%) and myalgia (17% vs 11%) on admission, although these differences were not significant.
Patients with gastrointestinal sequelae became ill less frequently than those without gastrointestinal sequelae (17% vs 37%; p = 0·021), although after adjustment for confounding factors, this difference was not significant (p = 0·051) .
Patients with gastrointestinal sequelae at 90 days had a lower frequency of supplemental oxygen therapy (79% vs 94%; p = 0·016), and a trend towards lower frequency of admission to the intensive care unit during hospitalization.
Patients with gastrointestinal sequelae at 90 days were treated more frequently with proton pump inhibitors (PPIs) and corticosteroids and were less frequently treated with enteral nutrition than patients without such sequelae (appendix p. 4-5).
Gastrointestinal sequelae including loss of appetite, nausea, acid reflux, and diarrhea are common in patients 3 months after discharge from COVID-19 hospitalization.
Persistent gastrointestinal symptoms have important implications for the appropriate management of patients and healthcare resources. Our data highlight the importance of gastrointestinal care and nutritional support for patients discharged after COVID-19 hospitalization.
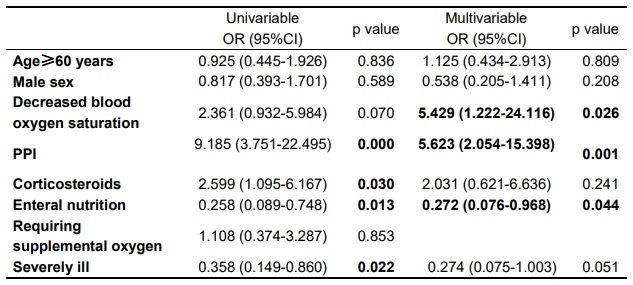
Univariate and multivariate logistic regression analysis on the associations between gastrointestinal sequelae and possible risk factors. OR = odds ratio. CI = confidence interval. Multivariable logistic regression was adjusted for age, sex, decreased blood oxygen saturation, treatments with PPIs, corticosteroids, and enteral nutrition, and severe illness.
The fact that severe illness during hospitalization was not associated with post-discharge gastrointestinal sequelae was unexpected. Decreased blood oxygen saturation , a symptom closely related to severe pneumonia, was found to be associated with gastrointestinal sequelae. This association could imply that hypoxia mediates the multiorgan injuries frequently seen with COVID-19.
It is important to note that hypoxia not only occurs in COVID-19 patients with dyspnea, but also in many patients without dyspnea.
Asymptomatic hypoxemia could explain the apparent discrepancy in our observation that decreased blood oxygen saturation, but not severe disease, is associated with gastrointestinal sequelae.
PPIs were often used for aspiration prophylaxis in patients admitted for suspected COVID-19 receiving anesthesia, parenteral nutrition, or other acid-related treatments. Acid rebound is a known consequence of PPI deprescribing, so it might be expected that PPI treatment during hospitalization would be associated with acid reflux after discharge.
Nutritional interventions during hospitalization appeared to be associated with a lower incidence of subsequent gastrointestinal sequelae. Up to 78% of patients hospitalized with COVID-19 report poor appetite. In addition to poor appetite, other common gastrointestinal symptoms such as nausea, vomiting, and diarrhea during hospitalization can lead to malnutrition , which has been linked to increased mortality in patients with COVID-19.
Nutritional support could be essential to maintain patients’ lives.
The reduction in gastrointestinal sequelae is probably part of the overall benefit of nutritional support.
Our study has several limitations . Being retrospective , data were missing for several relevant blood biochemical tests, such as blood markers for inflammation and serum SARS-CoV-2 titers. Another important limitation was that only 71% of discharged patients had sufficient data to be included in this analysis, which could lead to biased conclusions. Reliance on patient recall of symptoms during follow-up is another potential limitation. A prospective study will provide a better understanding of the long-term gastrointestinal sequelae of COVID-19.
We declare that there are no competing interests. This work was partially supported by the “Pearl River Talent Plan” Innovation and Entrepreneurship Team Project of Guangdong Province 2019ZT08Y464 (to LZ), National Natural Science Foundation of China grants 81770571 (to LZ) and 81774152 (to RZ ), the Special Project for Scientific and Technological Development and Emergency Response in COVID-19 Prevention and Control Grant of Guangdong Province 2020A111129028 (to LS), the Special Project for the Research and Promotion of COVID-19 Prevention and Control Techniques COVID-19 and emergency response in Dongguan City grant 202071715001114 (to LS) and the National Key Clinical Discipline of China.















